THE FLOW VOLUME LOOP
Winston
Your interest in medicine outside of your specialty continues to surprise me. Yes, on a number of occasions I have mentioned the importance of the flow volume loop in testing lung functions. It has remained an interest of mine throughout my medical career. I am sure I can provide much more information than you want to know, as I was present at its birth for general use as a clinical test.
The flow volume loop is a gift to the physician. An understanding of its secrets gives the knowledgeable practitioner a world of information. It can explain or help to explain the symptoms of dyspnea and other breathing complaints. Careful review reveals more profound secrets: the unacknowledged secrets of how to understand expiratory flow, and its problems.
My love affair with the flow volume loop began in 1974 when I was made head of the pulmonary function laboratory at Walter Reed Army Medical Center. I was a newbie in the world of pulmonary physiology. Yes, I was a fully trained, knowledgeable and soon to be board certified pulmonary specialist. But the world of physiology was a whole different category of knowledge, information and details – more than any trained pulmonary physician would possess after their training in the specialty. Furthermore, I was following in the footsteps of doctors who had been more thoroughly trained in pulmonary physiology; Sidney Braman and Robert Senior, both of whom went on to extraordinary careers in academic medicine.
Drs. Hyatt and Black had just published on the value of the flow volume loop as a measurement to diagnose airflow obstructions in the trachea and larynx. The flow volume loop had not been part of our education and most patient testing facilities were not set up to make those measurements, the Walter Reed Pulmonary Testing Laboratory included. That time was before the computation of medical testing and widespread computer use in general. Flow and volume lung tests were done manually and the flow volume loop was not available to the clinician. Fortunately, or unfortunately, it is now present on almost every commercial device that measures expiratory airflow. I believe that by being so widely available, their value is being overlooked.
The technology of the 70s was evolving rapidly. Physicians were trained to understand expiratory volumes and their timing. They were also instructed in measuring basic gas changes in the blood, lung size in health and disease and the ability of gas to enter the bloodstream. These measurements were rapidly becoming common tools in the practice of clinical medicine; so too, would the new test of lung function, the flow volume loop.
Physiologists in pulmonary research had learned to measure the speed or velocity of flow with the device called a pneumotact. It provided an instant electronic signal that reflected the velocity of flowing air. Prior to that ability, volumes were measured manually and flow calculated indirectly from paper recordings. The pneumotact could be calibrated to measure the speed with which air was moving. In the 1970s this was cutting edge. Now, over 50 years later, much cheaper, more stable and reliable but similar types of devices can perform the same function and are widely available for clinical use. Almost every device currently available to measure expiratory airflow does it with some sort of electronic measurement.
The volume of air exhaled traditionally had been measured by the displacement that air would cause into a sealed container. As the air changed the position of the container, it would create a mark on paper. The inscribed marks could be physically measured and the volume of air calculated. This volume displacement was developed in the late 19th and early 20th century. In the mid 20th century, the time it took to exhale the air into the container was added as a measure of lung function. Spirometry, as it was named, had been the only pulmonary function test for measuring aspects of lung function through the 20th century and remains a mainstay of lung testing in clinical medicine today.
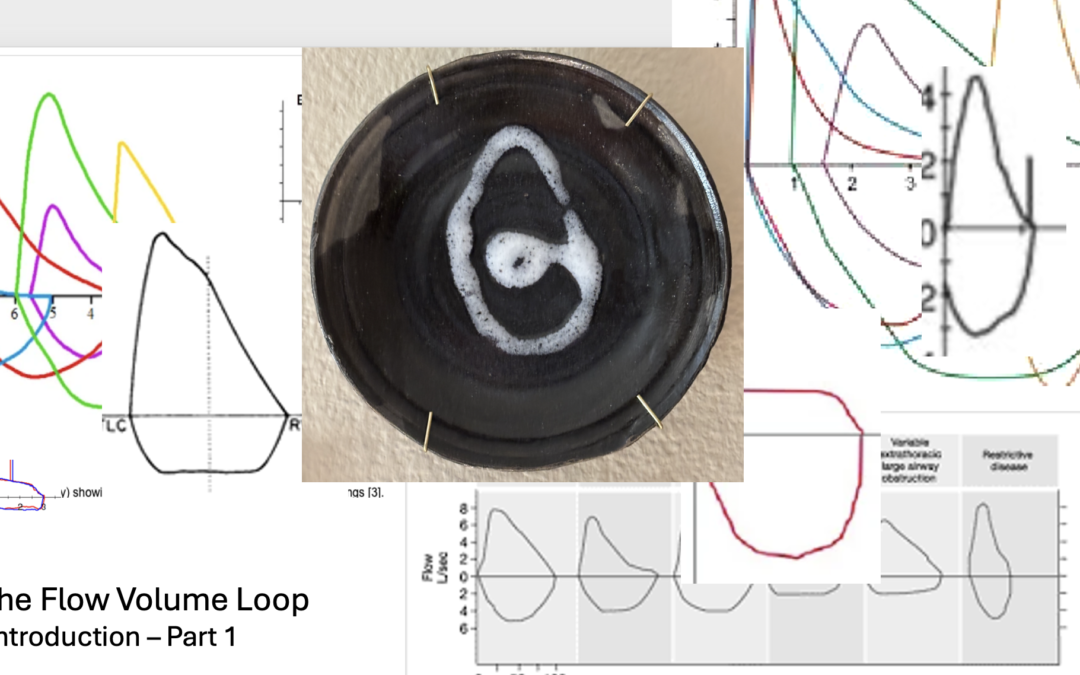
As a neophyte in the world of physiology, I was both frustrated and fascinated by the problems of measuring and using the flow loop. Reports by Miller and Hyatt, and then Black and Hyatt, chose to display the two parameters on an XY axis. These values needed to be measured simultaneously and plotted one verses the other. It could be projected on an oscilloscope (think of a digital screen with a line drawn on it) or on a special paper recorder. Traditionally, with spirometry testing of expiratory airflow, clinical test parameters evaluated were measurements of time on one axis and volume on the other. Those were the manually measured values. The addition of the simultaneous measurements of flow and volume, as well as the change in how they were presented, made the flow volume loop unique.
For other reasons, the lab at Walter Reed was well equipped. Previous directors had requested and received pneumotacts for use with other studies. They provided a way for me to measure the flow portion of the test. Within a few months, I was able to obtain the appropriate devices to measure volume and the special x-y recorder needed. With more than a little help from my knowledgeable staff, we created a digital signal for volume, flow, and time and then recorded them on the x-y recorder. I soon incorporated our measurement of the flow volume loop as a clinical tool. In the late 70s, subsequent upgraded testing equipment simplified these. But always in the back of my mind, those early tools brought joy to my reviews of the flow volume tests in my work.
As you can see Winston, in a relatively short period of time I was able to make the flow volume loop a clinical test available as part of the pulmonary function studies. But that was just the beginning.
Let me know if you desire more information. If you do, it may open Pandora’s flow volume box. If so, I think you would find it an interesting and valuable container.
Robert E. Hyatt MD and Black LF
Am Rev Respir Dis. 1973 Feb;107(2):191-9. doi: 10.1164/arrd.1973.107.2.191
RGH WeWi43,29,615
