Your interest in medicine outside of your specialty continues to surprise me. Yes, on a number of occasions I have mentioned the importance of the flow volume loop in testing lung functions. It has remained an interest of mine throughout my medical career. I am sure I can provide much more information than you want to know, as I was present at its birth for general use as a clinical test.
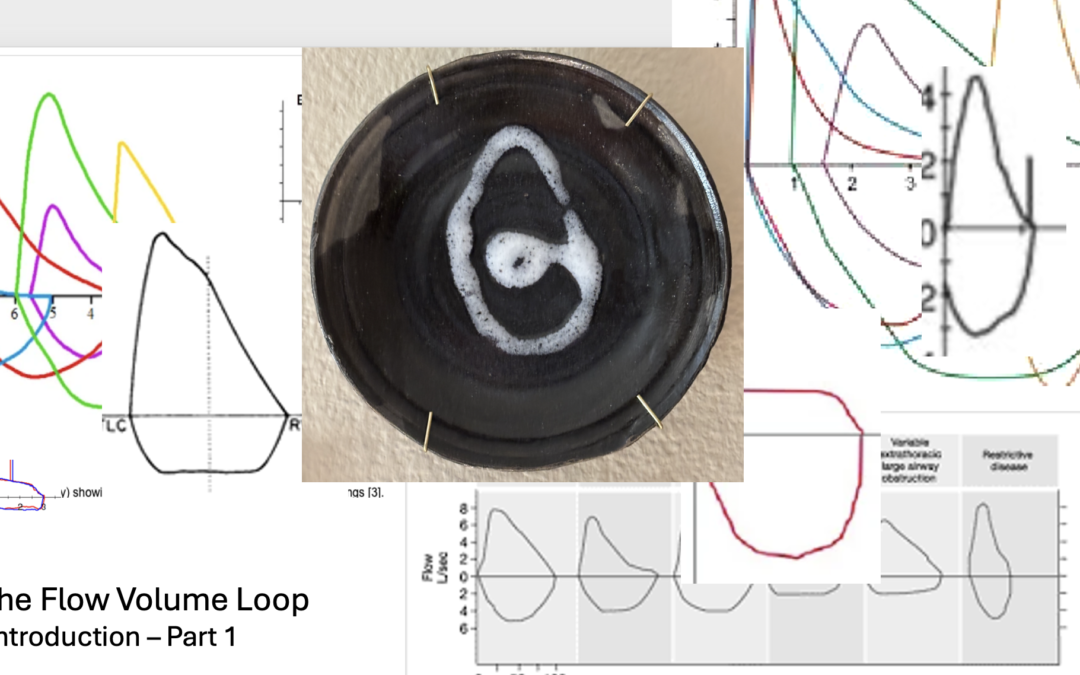
The flow volume loop is a gift to the physician. An understanding of its secrets gives the knowledgeable practitioner a world of information. It can explain or help to explain the symptoms of dyspnea and other breathing complaints. Careful review reveals more profound secrets: the unacknowledged secrets of how to understand expiratory flow, and its problems.
My love affair with the flow volume loop began in 1974 when I was made head of the pulmonary function laboratory at Walter Reed Army Medical Center. I was a newbie in the world of pulmonary physiology. Yes, I was a fully trained, knowledgeable and soon to be board certified pulmonary specialist. But the world of physiology was a whole different category of knowledge, information and details – more than any trained pulmonary physician would possess after their training in the specialty. Furthermore, I was following in the footsteps of doctors who had been more thoroughly trained in pulmonary physiology; Sidney Braman and Robert Senior, both of whom went on to extraordinary careers in academic medicine.
Drs. Hyatt and Black had just published on the value of the flow volume loop as a measurement to diagnose airflow obstructions in the trachea and larynx. The flow volume loop had not been part of our education and most patient testing facilities were not set up to make those measurements, the Walter Reed Pulmonary Testing Laboratory included. That time was before the computation of medical testing and widespread computer use in general. Flow and volume lung tests were done manually and the flow volume loop was not available to the clinician. Fortunately, or unfortunately, it is now present on almost every commercial device that measures expiratory airflow. I believe that by being so widely available, their value is being overlooked.
The technology of the 70s was evolving rapidly. Physicians were trained to understand expiratory volumes and their timing. They were also instructed in measuring basic gas changes in the blood, lung size in health and disease and the ability of gas to enter the bloodstream. These measurements were rapidly becoming common tools in the practice of clinical medicine; so too, would the new test of lung function, the flow volume loop.
Physiologists in pulmonary research had learned to measure the speed or velocity of flow with the device called a pneumotact. It provided an instant electronic signal that reflected the velocity of flowing air. Prior to that ability, volumes were measured manually and flow calculated indirectly from paper recordings. The pneumotact could be calibrated to measure the speed with which air was moving. In the 1970s this was cutting edge. Now, over 50 years later, much cheaper, more stable and reliable but similar types of devices can perform the same function and are widely available for clinical use. Almost every device currently available to measure expiratory airflow does it with some sort of electronic measurement.
The volume of air exhaled traditionally had been measured by the displacement that air would cause into a sealed container. As the air changed the position of the container, it would create a mark on paper. The inscribed marks could be physically measured and the volume of air calculated. This volume displacement was developed in the late 19th and early 20th century. In the mid 20th century, the time it took to exhale the air into the container was added as a measure of lung function. Spirometry, as it was named, had been the only pulmonary function test for measuring aspects of lung function through the 20th century and remains a mainstay of lung testing in clinical medicine today.
As a neophyte in the world of physiology, I was both frustrated and fascinated by the problems of measuring and using the flow loop. Reports by Miller and Hyatt, and then Black and Hyatt, chose to display the two parameters on an XY axis. These values needed to be measured simultaneously and plotted one verses the other. It could be projected on an oscilloscope (think of a digital screen with a line drawn on it) or on a special paper recorder. Traditionally, with spirometry testing of expiratory airflow, clinical test parameters evaluated were measurements of time on one axis and volume on the other. Those were the manually measured values. The addition of the simultaneous measurements of flow and volume, as well as the change in how they were presented, made the flow volume loop unique.
For other reasons, the lab at Walter Reed was well equipped. Previous directors had requested and received pneumotacts for use with other studies. They provided a way for me to measure the flow portion of the test. Within a few months, I was able to obtain the appropriate devices to measure volume and the special x-y recorder needed. With more than a little help from my knowledgeable staff, we created a digital signal for volume, flow, and time and then recorded them on the x-y recorder. I soon incorporated our measurement of the flow volume loop as a clinical tool. In the late 70s, subsequent upgraded testing equipment simplified these. But always in the back of my mind, those early tools brought joy to my reviews of the flow volume tests in my work.
As you can see Winston, in a relatively short period of time I was able to make the flow volume loop a clinical test available as part of the pulmonary function studies. But that was just the beginning.
Let me know if you desire more information. If you do, it may open Pandora’s flow volume box. If so, I think you would find it an interesting and valuable container.
Robert E. Hyatt MD and Black LF
Am Rev Respir Dis. 1973 Feb;107(2):191-9. doi: 10.1164/arrd.1973.107.2.191
I know it’s been a while. You haven’t heard from me in several months. Yes, I have been busy. I will try to communicate more often. First, I want you to know that all is well. Three major, well, time consuming and not ordinary events have occupied my last few months. I have completed two major projects and terminated a third.
Last summer I took extra time off from my clinical work at the Mayo. Planning ahead, I returned to it in the Fall. You will remember I was practicing part time to assist them with their backload of sleep patients. Interestingly to me, patient care is just as rewarding now as it was those years ago when I entered medicine. As they say, “You meet the nicest people.”
Computerization has ruined patient care. No, that is not exactly true. Computers have been a blessing. It is the multiple layers of regulations that are imposed through the computer programs and programmers that the doctor is burdened with completing. Large organizations are constantly modifying their systems to adjust to changing rules and regulations. I find those burdensome and onerous.
Returning to my patient care this Fall, I found it was clearly time to leave practicing clinical medicine with Mayo. My last day in September was sad but totally uneventful. So, I am officially working on my own. It is unlikely I will return to a clinical practice, but more details will follow and I will post them on the website.
“What about the other two projects?” you might wonder. They are a paper submitted and a book completed. I doubt the paper will have much success being accepted, as it is a consideration for the medical aristocracy suggesting that the AHI be modified by using total sleep time as part of the assessment for obstructive sleep apnea. I expect that I will need to offer it to another two or three journals before it is accepted for publication. Who knows, I might end up having to publish it on my own website which is certainly not the most prestigious thing to do.
And then there is the book, Reflections on Being a Physician. Depending on how I consider it, the project has lasted between three and 45 years. The book was released January 20, 2026. It is a series of essays describing the trials and tribulations I associated with becoming a physician, a series about the business of medicine from a physician’s point of view and lastly, and probably most importantly, my definition or perception of the differences between a physician and a doctor. I will send you a copy. I hope you find it an interesting read. It will be available through the website at a discounted price and available through book stores and online book retailers.
One point the book stresses is the need for doctors, physicians, nurse practitioners and physician assistants, all of us who are defined as practitioners by our government, to review and recommit ourselves yearly to our oath as a provider. It is a thought you should consider.
I will get to your other questions on my next note.
You didn’t ask for this. You probably do not even want it. Yes I know, but I promised you a primer on how to apply the qualitative and quantitative analyses of insomnia complaints. Remember, insomnia as a complaint can represent many different issues. These include difficulty going to sleep and staying asleep as well as going back to sleep after awakening or combinations of those issues. Before you can apply that information, you need a simple overview of how to consider the multiple factors that can produce difficulty with sleep.
The approach I find most helpful is based on general factors known to often cause difficulty with sleep. The categories along with a brief description are:
ENVIRONMENTAL: Environmental causes are usually recognized by the patient, but not always. Factors such as pets, spouses, lighting, thermostat settings and others are some reasons people do not sleep well.
MEDICAL: At some point almost all medical conditions may interfere with sleep. Frequent conditions are usually muscular skeletal such as injuries and arthritis. Other common, though short-term, issues include allergies and upper respiratory illnesses.
MEDICATIONS: You are not surprised to see medications, are you? Their side effects on sleep is an obsession of mine. A careful review is in order. The website has a listing under the medication tab of those and of those that frequently cause excessive sleepiness and sleeplessness.
PSYCHOLOGICAL: We all experience short term stresses and emotional upheavals that lead to anxiety and depression. Long term difficulties with insomnia can result from persistent problems with anxiety and depression. Similarly, anxiety and depression can cause difficulties with sleep. The degree of anxiety and depression needed to produce these complaints is of a magnitude that should be apparent to the patient and a perceptive doctor, though psychological issues are often difficult to assess.
HABITS: Habits can produce insomnia. Familiar to all, caffeine containing products lead the list. Less well-known dietary factors are alcohol, tea and chocolate. Not for their caffeine, but for other components. The activities a person pursues prior to sleep also can play a significant role. Food, drink, exercise, TVs and computers and lighting need reviewing.
STRUCTURE: Sleep structure refers to timing of sleep. What is the patient’s sleep duration and their time spent in bed trying to sleep? How long does the patient sleep when he sleeps well? Is the patient a night owl (likes to stay up late and wake late) or a lark (likes to go to bed early and wake early)? Are the sleep hours stable or do they change on weekends. Does the patient do shift work? How much sleep does this patient actually need? All these are factors that need to be considered.
SLEEP DISORDERS: The last category of potential issues are the disorders of sleep. Recognized disorders of sleep may produce difficulty with what a patient considers insomnia. For example, obstructive sleep apnea, thought to occur in 25% of all adults, can cause difficulty with sleep maintenance but rarely causes difficulty with initiating sleep. Restless legs and periodic limb movements need to be considered when insomnia is reported. Primary insomnia, insomnia without a known cause, is a diagnosis under this group.
Applying a qualitative and quantitative assessment allows the doctor to focus on specific areas of concern. Often, a provider will consider a patient to have primary insomnia without giving the other factors consideration. They take the patient’s complaints of insomnia – the patient’s perceptions of their sleep difficulties as insomnia – to be insomnia without a cause and proceed with medications to help induce sleep. Getting needed information from the patient is often difficult and time can limit the providers’ opportunities to explore other possible issues. For example, frequently a patient will tell me they have stopped using caffeinated products, but upon questioning, tea or energy drinks are still being used. Another major issue is medications. Patients may be on multiple medications which can produce sleeplessness or sleepiness. It can be impossible at times to separate their specific effects.Clearly identifying the details of the complaint will direct the provider to specific items to be considered for the patients diagnosis and treatment.
It is possible to identify contributing or causative factors in many patients with insomnia complaints. The qualitative and quantitative assessments often lead to specific addressable issues that can be modified or treated without the use of sleep-inducing medications. My working patterns can be summarized best in a tabular form that I have reproduced below.
When a patient’s complaints fall into one of these patterns, a more detailed history and investigation to assess that issue will follow.
And yes, Winston, I will try not to bother you with any more advice on insomnia.
RGH 29430
COMMON PATTERNS OF INSOMNIA COMPLAINTS IN SPECIFIC SLEEP PROBLEMS
Yes, that is what I said; “A problem with insomnia needs to be analyzed qualitatively.”
During my college years, I majored in the study of chemistry. The study requirements included courses in qualitative and quantitative analysis. Essentially, the study of what a substance is made of and how much of each component part is included. My comment on analyzing insomnia qualitatively means that a physician should know the components of the complaint.
The term, insomnia, has a multitude of meanings in common use as well as in medicine. The physician needs to know what the person using the term is experiencing. In essence, what are the specific issues involved? It is only with this type of clarity that the patient’s situation can be assessed. The analysis includes the effects on daytime activities and is designed for nocturnal sleepers. Those whose primary sleeping time is during the day, for example shift workers, require a different approach.
Difficulty falling asleep or initiating sleep is the most recognized problem described by the term. Defining the time required for sleep onset is the first step in assessing insomnia. A problem with sleep initiation may be someone’s sole issue or it may be just one part of the patient’s problem.
Another difficulty often described as insomnia is waking frequently during the sleep period. It is common and considered normal to wake once or twice a night. Waking more often disrupts sleep and is frequently an issue for the patient. Those with this complaint may or may not have a third type of problem, returning to sleep.
Returning to sleep after waking during your night of sleep, can be a singular issue or can be associated with other insomnia issues. Some will wake frequently while others will wake only once or twice. A problem returning to sleep can occur in either situation.
Waking earlier than desired is another issue commonly reported as insomnia. All of these complaints may occur independently or in combination with one or more of the others.
Knowledge of the effects of the sleep problem on daytime wakefulness and napping is helpful diagnostically. Is the person sleepy during the day? Do they nap? Do they nod off?
To analyze complaints of insomnia, a physician needs to understand:
Are there problems with sleep initiation?
Are there problems with sleep maintenance?
Are there problems with returning to sleep after awaking?
Are there problems with waking too early for the day?
Are there problems with daytime sleepiness?
A patient’s historical ‘insomnia qualitative profile’ information is required for accurate assessment. Unfortunately, getting the information can be difficult, time consuming and even impossible. When obtainable, it will help with establishing a diagnosis, but a pattern of difficulty does not indicate a specific reason or cause for the issues. In fact, many or most individuals will have more than one potential causative or aggravating issue.
The frequency the symptoms occur and their intensity are important in narrowing the potential reasons or contributing factors to the sleeplessness problem. How significant is each of the symptoms reported? This step is the quantitative analysis of each of these factors
Diagnostic considerations of insomnia require knowledge of the specific complaints (the qualitative analysis) and the degree to which they are present (the quantitative analysis) for assessing factors that are known to produce insomnia.
So Winston, I have returned to my youth of qualitative and quantitative analysis. A famous troubadour once penned a song; “All my life’s a circle, sunrise to sunset.” So it appears to be. I suspect this is more than you probably wanted to know. Maybe I should prepare a short primer for you on the roles of the qualitative and quantitative assessments in identifying the factors, conditions and behaviors known to produce and aggravate insomnia.
Once I lost a hammer. It was a tool I earned in my youth while working to finance my education. It taught me to respect the tools I use in my work. On a past occasion (30 years ago), I wrote how doctors should view their tools: a major one being hospitals. My hope was that practicing doctors would work to influence those institutions for the better. Oh, such were the dreams of my youth. Hospitals are now conglomerates operated by boards and individuals steeped in the profit motives common to all corporations. These are boards and individuals who are far removed from our Oath. They are focusing on the growth and profit for the corporate owners, not on a profit to benefit the community, patients, employees, operations and doctors that it serves. It is a tool that I believe is lost for the lifetime of most current doctors. Now a newer tool already widely used is my current concern: the electronic medical record.
This story begins with my Apple IIe. No, it actually begins much earlier than that. It begins my senior year in high school. An opening in my class schedule allowed me to choose a class of my choice. I chose typing. As a result, I had the advantage of being able to type in college, medical school and even now. My time in high school was before electric typewriters and computers. Since I could type, buying my IIe let me explore the world of computing. It was great fun and allowed me to explore simple basic programing, even writing a program for the interpretation of blood gas test results. Within a short time, professional programers were producing much more sophisticated versions. My skills were in the medical, not the computer field. I need not burden you with the progress in the computer world.
As my medical practice matured, my use of computers kept up with their ability to make life easier. My specialty practice needed quality reports to keep its referring physicians informed as did my work interpreting hospital studies. The computers of the 90’s and since, allow for the creation of these. More ominously, the financial aspects of medical practices began to require computerization. Progress in technology and increased control over fees and payments by outside businesses and government required more and more computerization. Then, a little more than a decade ago, the electronic medical record appeared. It first was a way to organize the doctor’s medical files, but integration with the financial aspects of practice rapidly followed. The electric, digital medical record was born. Hospital and medical practices, with significant government encouragement, widely adopted the electronic system. Use became mandatory for some.
“Open the Pod Bay doors, Hal.” Requested astronaut Dave Bowman.
“I’m sorry, Dave. I’m afraid I can’t do that.” Responded Hal, the 9000 Computer
“The X system does not allow that. I think you can work around it. You will need to go to the ‘order’ tab, then the ‘misc’ tab. That will get the dropdown menu for other items. It is probably listed there.” The support staff cheerily reviewed for me. Their acceptance of the complexities of the digital medical record is probably based upon their knowledge of its inner working. Most of the staff were born after my IIe was manufactured. Raised with and around computers, their acceptance of these difficulties is as understandable as it is disturbing. Though their followup comment indicates dependency on a higher authority, “Sharon, Medical Record X’s representative, can probably help us with that. I will reach out to her. I can have something for you in a few days.” This interaction has become more and more common when a doctor working for a large group or organization runs into issues with documenting, placing orders or communicating with their patients.
Don’t misunderstand me. They are trying to be helpful. They definitely know more about the X electronic medical record than the physicians do. What is irritating is their acceptance that it is the holy grail of records. Their entire lives have been during the computer age. It leads them to accept all its faults and I suspect, to not fully understand why just a few more clicks to memorize and perform does not leave me happy. What happens when the business Medical Record X changes the clicks, deletes the item or task needed or I forget the clicks? I am back to square one.
“Dave, this conversation can serve no purpose any more. Goodbye,” concludes Hal when it tires of discussing opening the pod bay doors with Dave. Hal has made a decision and it will not change. Dave will be left in space. Dave using human ingenuity ultimately finds an alternate way back into the space craft.
Recently it was announced, company X had added an upgrade that some of the support staff were using. It is a program to change a prepared patient message to a calmer more comforting tone and words. We were told it has helped improve the patient’s perception of a few of the staff messages where it has been used. How does it work? A message is prepared. You ask the program to review it. It does, and then changes how the message is phrased and addressed the patient. Red flags flew in my head. Is it the first step in eliminating the human contact in medical care? For example, just feed the result of a test to the system and it prepares and sends the message. Will it become similar to the multitude of robo calls, messages and commercial computer chats to which we are now exposed? Yes, I am being a bit paranoid. At the least, it does indicate some of the support staff need to improve their communication skills.
“Just what do you think you’re doing, Dave?” Hal asks.
“Dave, stop. Stop, will you? Stop, Dave. Will you stop Dave? Stop. Dave.” Hal attempting to stop Dave from deactivating it.
Hal’s finial vocalizations, “I’m afraid. I’m afraid. Dave. Dave my mind is going. I can feel it. I can feel it. My mind is going.”
Dave completed his mission without Hal. Following Dave’s guidance, maybe we need to disable X. No, that would be like doing away with the car, a terrible thought. Without the automobile, modern society would crumble. There are cars made to go 180 miles per hour and travel through deserts and mountains with ruts for roads, but few will purchase them and even fewer use those features. Unfortunately, the typical electronic medical record system comes with the 180 mile per hour and off-road options. Unlike the car of your choice, you are more a passenger than the driver of the record.
Those options on the electronic record are controls that constrain the medical practice to conform to insurance and government standards. We should recognize the dangers of its controlling nature. It is very similar to government. Governments have an essential role in allowing a free society to flourish and too much government results in tyrannical control. In our era, China, North Korea, Cuba and Russia are good examples of too much control. The computer has an important, almost essential role in medicine, but when controlled by self-interested parties, it can become tyrannical.
As the ultimate users, doctors, and maybe patients, need to police the features included in the computerization of the medical record. Let’s not buy those controlling features. Remember, your role in most systems will be that of passenger, not driver, and it is going to be a long, frustrating, expensive ride.
*From “2001, A Space Odyssey,” a movie by Stanley Kubrick released in 1968 to mixed reviews. Now considered one of the greatest and most influential films ever made. These quotes are taken from a section of the movie on a space voyage from Earth to Jupiter where Hal, the human like computer controlling the flight and the space craft, has locked the human astronaut out of the space craft and refuses to let him back in. You see, Hal had made a mistake and could not admit it. How very human like.