You didn’t ask for this. You probably do not even want it. Yes I know, but I promised you a primer on how to apply the qualitative and quantitative analyses of insomnia complaints. Remember, insomnia as a complaint can represent many different issues. These include difficulty going to sleep and staying asleep as well as going back to sleep after awakening or combinations of those issues. Before you can apply that information, you need a simple overview of how to consider the multiple factors that can produce difficulty with sleep.
The approach I find most helpful is based on general factors known to often cause difficulty with sleep. The categories along with a brief description are:
ENVIRONMENTAL: Environmental causes are usually recognized by the patient, but not always. Factors such as pets, spouses, lighting, thermostat settings and others are some reasons people do not sleep well.
MEDICAL: At some point almost all medical conditions may interfere with sleep. Frequent conditions are usually muscular skeletal such as injuries and arthritis. Other common, though short-term, issues include allergies and upper respiratory illnesses.
MEDICATIONS: You are not surprised to see medications, are you? Their side effects on sleep is an obsession of mine. A careful review is in order. The website has a listing under the medication tab of those and of those that frequently cause excessive sleepiness and sleeplessness.
PSYCHOLOGICAL: We all experience short term stresses and emotional upheavals that lead to anxiety and depression. Long term difficulties with insomnia can result from persistent problems with anxiety and depression. Similarly, anxiety and depression can cause difficulties with sleep. The degree of anxiety and depression needed to produce these complaints is of a magnitude that should be apparent to the patient and a perceptive doctor, though psychological issues are often difficult to assess.
HABITS: Habits can produce insomnia. Familiar to all, caffeine containing products lead the list. Less well-known dietary factors are alcohol, tea and chocolate. Not for their caffeine, but for other components. The activities a person pursues prior to sleep also can play a significant role. Food, drink, exercise, TVs and computers and lighting need reviewing.
STRUCTURE: Sleep structure refers to timing of sleep. What is the patient’s sleep duration and their time spent in bed trying to sleep? How long does the patient sleep when he sleeps well? Is the patient a night owl (likes to stay up late and wake late) or a lark (likes to go to bed early and wake early)? Are the sleep hours stable or do they change on weekends. Does the patient do shift work? How much sleep does this patient actually need? All these are factors that need to be considered.
SLEEP DISORDERS: The last category of potential issues are the disorders of sleep. Recognized disorders of sleep may produce difficulty with what a patient considers insomnia. For example, obstructive sleep apnea, thought to occur in 25% of all adults, can cause difficulty with sleep maintenance but rarely causes difficulty with initiating sleep. Restless legs and periodic limb movements need to be considered when insomnia is reported. Primary insomnia, insomnia without a known cause, is a diagnosis under this group.
Applying a qualitative and quantitative assessment allows the doctor to focus on specific areas of concern. Often, a provider will consider a patient to have primary insomnia without giving the other factors consideration. They take the patient’s complaints of insomnia – the patient’s perceptions of their sleep difficulties as insomnia – to be insomnia without a cause and proceed with medications to help induce sleep. Getting needed information from the patient is often difficult and time can limit the providers’ opportunities to explore other possible issues. For example, frequently a patient will tell me they have stopped using caffeinated products, but upon questioning, tea or energy drinks are still being used. Another major issue is medications. Patients may be on multiple medications which can produce sleeplessness or sleepiness. It can be impossible at times to separate their specific effects.Clearly identifying the details of the complaint will direct the provider to specific items to be considered for the patients diagnosis and treatment.
It is possible to identify contributing or causative factors in many patients with insomnia complaints. The qualitative and quantitative assessments often lead to specific addressable issues that can be modified or treated without the use of sleep-inducing medications. My working patterns can be summarized best in a tabular form that I have reproduced below.
When a patient’s complaints fall into one of these patterns, a more detailed history and investigation to assess that issue will follow.
And yes, Winston, I will try not to bother you with any more advice on insomnia.
RGH 29430
COMMON PATTERNS OF INSOMNIA COMPLAINTS IN SPECIFIC SLEEP PROBLEMS
Yes, that is what I said; “A problem with insomnia needs to be analyzed qualitatively.”
During my college years, I majored in the study of chemistry. The study requirements included courses in qualitative and quantitative analysis. Essentially, the study of what a substance is made of and how much of each component part is included. My comment on analyzing insomnia qualitatively means that a physician should know the components of the complaint.
The term, insomnia, has a multitude of meanings in common use as well as in medicine. The physician needs to know what the person using the term is experiencing. In essence, what are the specific issues involved? It is only with this type of clarity that the patient’s situation can be assessed. The analysis includes the effects on daytime activities and is designed for nocturnal sleepers. Those whose primary sleeping time is during the day, for example shift workers, require a different approach.
Difficulty falling asleep or initiating sleep is the most recognized problem described by the term. Defining the time required for sleep onset is the first step in assessing insomnia. A problem with sleep initiation may be someone’s sole issue or it may be just one part of the patient’s problem.
Another difficulty often described as insomnia is waking frequently during the sleep period. It is common and considered normal to wake once or twice a night. Waking more often disrupts sleep and is frequently an issue for the patient. Those with this complaint may or may not have a third type of problem, returning to sleep.
Returning to sleep after waking during your night of sleep, can be a singular issue or can be associated with other insomnia issues. Some will wake frequently while others will wake only once or twice. A problem returning to sleep can occur in either situation.
Waking earlier than desired is another issue commonly reported as insomnia. All of these complaints may occur independently or in combination with one or more of the others.
Knowledge of the effects of the sleep problem on daytime wakefulness and napping is helpful diagnostically. Is the person sleepy during the day? Do they nap? Do they nod off?
To analyze complaints of insomnia, a physician needs to understand:
Are there problems with sleep initiation?
Are there problems with sleep maintenance?
Are there problems with returning to sleep after awaking?
Are there problems with waking too early for the day?
Are there problems with daytime sleepiness?
A patient’s historical ‘insomnia qualitative profile’ information is required for accurate assessment. Unfortunately, getting the information can be difficult, time consuming and even impossible. When obtainable, it will help with establishing a diagnosis, but a pattern of difficulty does not indicate a specific reason or cause for the issues. In fact, many or most individuals will have more than one potential causative or aggravating issue.
The frequency the symptoms occur and their intensity are important in narrowing the potential reasons or contributing factors to the sleeplessness problem. How significant is each of the symptoms reported? This step is the quantitative analysis of each of these factors
Diagnostic considerations of insomnia require knowledge of the specific complaints (the qualitative analysis) and the degree to which they are present (the quantitative analysis) for assessing factors that are known to produce insomnia.
So Winston, I have returned to my youth of qualitative and quantitative analysis. A famous troubadour once penned a song; “All my life’s a circle, sunrise to sunset.” So it appears to be. I suspect this is more than you probably wanted to know. Maybe I should prepare a short primer for you on the roles of the qualitative and quantitative assessments in identifying the factors, conditions and behaviors known to produce and aggravate insomnia.
Yes, yes, Winston, I have heard about the new medication approved by the FDA. It has been heralded as the first drug approved for the treatment of Obstructive Sleep Apnea. “Is it so?” you ask. It is, but as an infamous man once said, “It all depends on what the definition of is, is.”
The approval is the FDA giving it an indication for use in obese patients with moderate to severe obstructive sleep apnea. With that approval, it becomes the first medication to have an indication for use in Obstructive Sleep Apnea. This is the fact that has been in multiple news outlets and led to many questions of sleep doctors by our patients. It is important to know more about the details.
The approval followed a multi-million dollar, manufacture sponsored study that was published in the New England Journal of Medicine (NEJM). The study focused on using the weight loss drug in obese individuals with Obstructive Sleep Apnea. Unsurprisingly, the weight loss induced by the medication resulted in improvement in the apnea condition. The treated patients were compared to those treated by diet alone who lost little weight during the study. It was not compared to other weight loss drugs. The article received wide acclaim and attention.
What was known about excessive body weight, weight loss and Obstructive Sleep Apnea before this study? I have an interest in the subject and have followed the work in the field since seeing my first patient with sleep apnea while serving in the Army. He was thin as a rail, by the way. Current knowledge is that we know slightly more than half of all newly diagnosed apnea patients have problems with their weight. We know that of those patients who experience significant weight loss, apnea is eliminated in 18-20% of the obese patients. The others are usually improved, but apnea is not eliminated.
My review of the NEJM article can be summarized briefly. The drug causes weight loss (previously known) and the weight loss improved apnea in many with it. Does it work any better than weight loss by any other means: diet, counseling or other weight loss drugs? Who knows? The study does not address the issue. Does it improve apnea over and above the effect of losing weight? Who knows? The study does not address the issue.
What did the article do? I don’t think it provided any new information. It most likely – I speculate here – influenced the FDA to add the Sleep Apnea with obesity indication to the medication’s approved usage. I suspect that the several million dollars spent for the study resulted in far more notoriety and media attention than any amount of advertising money could buy. Additional facts for you to consider are the cost of the medication and the duration of treatment it requires. A quick Internet search shows it to cost between 900 and 1,000 dollars a month on a well-known discount site. The duration of treatment is potentially life long.
No Winston, it is not proven to be a drug for apnea: just another very expensive drug for weight loss.
Yes, I am aware of the national TV ads for the hypoglossal nerve stimulator for Obstructive Sleep Apnea. Earlier this year I prepared an information sheet on the subject. I will add it to this letter.
It is a second line therapy and works for a limited sub group of patients with Obstructive Sleep Apnea. CPAP is far more successful in controlling sleep apnea.
It primarily indicated for those who have failed CPAP. Unfortunately, there is no accepted definition what constitutes failing CPAP therapy. Reasons for stopping CPAP are many and sometimes complex. I have been intrigued by the issues that cause a patient to discontinue or be unable to use it and will add more on the subject on another occasion.
RGH 29.112 Sept 2023
Hypoglossal Nerve Stimulator (Inspire) May 2023
Device
“Inspire” is a device that senses an obstructive apneas and then sends a signal to the hypoglossal nerve through a wire. It activates the nerve, which causes the base of the tongue to move forward. The device, wires that sense the apnea and the wire from the device to the nerve are implanted under the skin. It is remotely controlled.
Candidates / Indications (Varies from FDA, Insurance and Medical societies)
Its primary indication for use is failure to be able to use CPAP. Problems with insomnia, restless legs or other sleep disorders must be controlled before being considered for Inspire. The obstructive apnea rating (apnea hypopnea index or AHI) on diagnostic testing should be between 15 and 65. Weight should be a BMI of under 32. BMI varies by height. For a 5’11” person a BMI of 32 is 225 lbs. Some insurances will allow a slightly higher BMIs. You must be older than 18 years of age. It is indicated when apnea obstruction occurs at the base of the tongue.
Cost
A rough estimate of the cost of the device, its implantation, testing and physician visits will be between forty and fifty thousand dollars.
Insurance Coverage
“Inspire” is a second line therapy and insurance companies only approve those who have failed other forms of treatment.
Process
If you meet the criteria for the device, you will be evaluated to see if the device will correct your apnea. The evaluation steps include a facility based sleep study, a sedated endoscopy of your upper airway and provider visits. Many will not fit the type of obstruction that the device will correct and will not be candidates.
If you are a candidate, then implantation, physician review and repeat testing to insure appropriate function will be required. These steps include surgery, a post activation facility based sleep study and provider visits.
The overall time from initial consideration to successful activation is about 5 to 6 months. Medical follow up currently is recommended every 6 to 12 months.
Results After Implantation
The goals of treating obstructive apnea are to reduce the AHI to less than 5 and to improve the quality of sleep. CPAP will achieve AHIs < 5 a very high percentage of the time. The Inspire device will reduce the AHI to less than 5 in approximately 50% of recipients. The rest will have a reduction in their AHIs but not to normal levels. Standard therapies such as CPAP may still be needed.
Other Considerations
“Inspire” is a man-made product with batteries. Wires can break. Wires cannot easily be removed. Batteries or new wires may be required in the future. There are a limited number of experienced physicians available to deal with the device. Other devices may still be needed and recommended to control your apnea condition.
It is inspiring to learn of your interest in sleep apnea. I will be happy to do my best to simplify, clarify and muddy your understanding of the AHI. AHI stands for Apnea Hypopnea Index. It is the standard for defining the presence of significant sleep disordered breathing and the condition of Obstructive Sleep Apnea.
It started long ago in the history of sleep medicine. In actual time, it was just 40-50 years ago. Physicians noted breathing problems during sleep. Over a decade or so it was clear from investigations that the problem was one of blockage of the airway in the throat during sleep. The blockage resulted in less air getting in and out of the lungs. The blood oxygen levels would drop, while the carbon dioxide level would increase. The sleeper responded with increased breathing efforts, which opened the airway. By the 1980’s, testing for these variables had evolved from investigative to the clinical practice level.
The AHI is the fundamental measurement for obstructive and central types of sleep disordered breathing. The A stands for apnea, or absence of breath. The H stands for hypopnea, or a critical reduction of airflow causing the same physiologic changes that the apnea produces. The I stands for index but actually represents a measurement of rate, the number of apneas and hypopneas per hour of sleep. The apnea as used in AHI represents the absences of air movement at the nose and mouth. Respiratory efforts by the diaphragm and chest may or may not be present. These are the simple definitions.
Clinicians and physiologists have much more specific definitions. Our definitions include the magnitude and duration of physiologic changes, as well as the types of equipment used for the measurements and the frequency of the changes. It should not surprise you that significant debate continues about the details of those changes. Opinions differ. Unfortunately, the efficient computerized testing systems we utilize, ease the burden of testing large numbers of people, but limit the ability to look at multiple variations of potential changes in definitions.
In this country, current technical definitions and the threshold for diagnosing the medical condition of apnea are cemented in place by the regulatory bodies; Medicare and commercial insurance companies set the standards. While the definitions set are supported by reported evidence, the standards are far from perfect and will not change soon.
The AHI is the gold standard for the definition of obstructive and central sleep apnea. Five events, apneas and or hypopneas, per hour of sleep meet diagnostic level for apnea. The level of 5 events was arrived at arbitrarily, based on early work in the field. Although accepted by those regulating groups, the actual minimal AHI needed to establish the diagnosis is not really known.
It is known that the higher the AHI the greater the risk for long-term medical problems. When a sleep study is complete and the AHI criteria for apnea is met, it is described as mild (5-15 events}, moderate (15-30 events) or severe (>30 events) apnea. The adjectives (mild, moderate and severe) represent the long-term risk for medical complications, not how a person feels. These separations into different severities of apnea, represent more tradition than science. In fact, the AHI is only a good predictor of severity for long-term complications at high levels (more complications) and very low levels (less complications). In the decades since these definitions for the onset and the severity of the disease were adopted, much research has been done. It appears that further definitions of these obstructive events would improve the accuracy of our diagnoses and the predictability of the future for the patient.
The current definitions have served time well. As a clinical tool, the AHI has proven to be extremely useful. It is accepted worldwide. Tremendous improvement in diagnosis and therapy for sleep apnea has occurred utilizing these measurements. There are limitations, however. This is specifically true when scientific studies of the condition are performed.
The role of low oxygen levels has been investigated more than any other factor. You will recall oxygen is measured on testing by the noninvasive transcutaneous method that reports oxygen saturations. Our technical definitions include a certain drop in oxygen saturation that is caused by the interruption to the airflow during the breathing events. The roles of the duration, severity and timing of the drop of oxygen in the sleep pattern as well as the total time spent at certain levels of oxygen desaturation are not known. Studies reviewing low oxygen levels during apnea suggest that the time spent with saturations of less than 90% together with the AHI is more accurate in predicting long-term medical complications than the AHI alone.
Another major factor not addressed with current testing is the use of a rate measurement for diagnostic purposes. A rate does not measure total exposure to apnea events. That is dependent on actual sleep time. An easy example is the difference of someone sleeping six hours versus another person who sleeps nine hours. They both can have the same AHI, but the person sleeping nine hours will be exposed to 50% more apnea events than the person who only sleeps six. The importance of exposure has not been studied at all.
The events we measure, apneas and hypopneas, do not occur uniformly throughout a night of sleep. The event frequency can change based upon body position. They can occur more while sleeping on the back verses the stomach. The events can occur more in REM sleep than in slow wave or Non-REM sleep. Research into the effects of these variables as predictors of long-term outcomes is limited.
Well, I believe it is time to close. The AHI is an immensely useful tool in the diagnosis and treatment of sleep apnea. It is the gold standard measurement for the diagnosis of sleep apnea. It needs to be improved upon and will be. As you will learn throughout your career, medicine changes slowly. Opinions are more rigid in medicine and in science than most believe. So, keep an open mind. This, like all things medical, will change with time.
There are complex airway dynamics resulting in blockage of the upper airway producing Obstructive Sleep Apnea. Although complex, the process can be viewed in a general non-technical manner to help one understand the causes of obstructive sleep apnea.
In such an overview, we find two components to the events producing blockage of the airway during sleep: airway muscle relaxation and airway size. How does each of these contribute to the development of obstructive apnea?
The basic event of sleep apnea is the relaxation of the upper airway (the throat above the Adam’s apple to the nose and mouth) narrowing it critically or totally, resulting in a blockage limiting the amount of air traveling into or out of the lungs. This causes a drop in the blood oxygen and an increase in the blood carbon dioxide. These are changes, which the brain notices immediately. The very next breathing effort by the diaphragm is stronger. These efforts keep increasing until two or three breaths later, on average about 15 to 20 seconds, the effort is strong enough that the throat opens and air moves in and out again. Commonly, but certainly not always, this is accompanied by a loud snore or snort. These events are what produce Obstructive Sleep Apnea.
While these events alone may not be medically important, they produce problems when they occur repeatedly. A measurement of five events per hour while sleeping is considered diagnostic of Obstructive Sleep Apnea in the United States. Problems are thought to develop at this point.
Relaxation of the tongue and pharyngeal muscles play a role in developing these events. As we age, muscle tone decreases. Strength reduces. Tissue tone becomes slack, to say the least. We have all seen the effects of age in our family, friends and maybe even ourselves. The same changes take place in our tongue, pharyngeal muscles and supporting tissues. The prevalence data for obstructive sleep apnea show a steady increase with age. Those greater than 70 years of age are reported to have an 80% frequency of occurrence.
Muscle relaxation and muscle changes with age are major components of the causation of obstructive apnea.
What role does airway size play in causing obstructive apnea? The size of the airway determines how much muscle relaxation is needed for the critical narrowing to occur. Smaller airways will close more easily than larger ones
It is best to look at the airway size as two issues – weight and genetics.
In the 1960s, doctors discovered and described the obstructive apnea problem in obese patients. For the first 20 years after its description, many strongly believed that obstructive apnea was just a complication of obesity, not an independent problem. When a person gains weight, the fat tissue is added over the muscles below the skin in most areas of the body, including under the skin in the throat. The accumulation in the throat makes the size of the airway smaller. With a smaller airway, less relaxation is required to cause the critical narrowing resulting in an obstructive apnea event.
It is now well known that at certain weights almost everyone will have apnea. The medical community uses a measurement that is a calculation based on height and weight. This is called the Body Mass Index or BMI. A normal BMI is 20 to 25. When a person’s BMI reaches 40, ninety percent of those individuals will have sleep apnea.
Obesity can cause sleep apnea. What is its contribution to all those individuals with the condition? No one agrees and there has been ongoing debate since the 1970s.
Like most medical controversies, variation in the reported studies makes the issue more difficult to understand.
Early attempts to understand the effects of weight loss on apnea used an improvement in symptoms as the mark of correcting the problem. When obese patients with apnea lose a significant amount of weight, they feel and sleep better. The authors of those reports concluded that obstructive sleep apnea was cured by weight loss. But, did it really cure the apnea?
As more studies were done, the investigators began testing for apnea after weight loss. To assess the effect of weight loss on correcting apnea, the reports used changes in patients’ sleep test measurements. Typically, they would use a percentage drop in the number of apnea events or select a set level of events at 15 or 5 per hour. The level of 5 is the diagnostic level accepted for the diagnosis of the condition. These studies report a high level of symptomatic improvement with weight loss. Unfortunately, only 10-15% of obese patients will drop their levels below 5 after weight loss. Most will reduce the number of events limiting the severity, but few can be considered as cured. For an individual, weight loss can have significant beneficial effects on treatment, need for treatment and symptoms. However, when viewed as a cause, few can be considered to have obstructive apnea caused by obesity.
My experience reported a few years ago at a community sleep center gives an insight. For every one hundred cases of newly diagnosed obstructive sleep apnea, 60 will have BMIs in the obese range, meaning that 60% were obese. After weight loss, we know only 10 to 15% of individuals will have their apnea event drop below 5 per hour. In the one hundred newly diagnosed individuals with apnea, weight loss will correct the apnea in only 6-10 of the 60 who had weight issues. The other 50- 54 previously obese now are of normal weight and still have apnea. They will feel better after weight loss, but they will still have apnea. There are now a total of approximately 90 who still have apnea. Why?
There is the problem of muscle relaxation of course, but there is the other component of airway size – Genetics.
Sleep doctors look at throats when evaluating their patients. As a practitioner for many years, I have looked at the throats of thousands of patients with obstructive apnea. How many abnormal throats have I observed? Not many. I have seen one throat malignancy in my last two thousand exams. By including enlarged tonsils and changes due to prior surgeries, the total would still be very low. Very few patients with apnea have abnormal throats. However, all throats ARE DIFFERENT.
As someone who looks at throats for a living, I can tell you that throats are like faces. They are all similar, but they are all different. Some have large tongues, some small jaws, some low palates, some high palates, some narrow throats, some wide, but all are different.
Our throats are part of our physical anatomy given to us by our parents. It is our genetic gift for life. There are an infinite number of combinations that might be expected. The easiest way to describe the effects of our anatomy and genetics on our throats is simply by the throat’s size. Some throats are large and some are small. Smaller throats have less room for the relaxation that occurs during sleep and as a result, obstructive apnea may occur at a younger age. A large throat may result in one never having the condition.
Over the past fifty years there are a variety of diseases and conditions that have been recognized as producing Obstructive Sleep Apnea. Severe hypothyroidism and acromegaly are examples. These are rare causes. They affect muscle relaxation and airway size in a variety of ways. Some ethnic groups have been shown to have a higher incidence of Obstructive Sleep Apnea – predominately those of Southeast Asian and black heritage. These increases are proposed to be secondary to the bony structure of the face and cranium reducing airway size in those populations.
So these are the factors that lead to obstructive apnea: age, muscle relaxation, weight and genetics. By the time we are in our 70s, most of us will suffer from the condition. It could almost be considered a part of the aging condition. Add in the genetic component and the weight factor, obstructive apnea can appear at a younger age.
SUMMARY:
Three Predominate Components To
The Development Of Obstructive Sleep Apnea
Muscle relaxation – Increases with Age
Airway size – Genetics
Airway size – Weight
The combination of the above factors in some proportion leads to the development of obstructive sleep apnea for the majority of affected individuals.
It is best to think of Obstructive Sleep Apnea as a potential companion you will share for life. Like grey hair and glasses for most, hearing aids for some, obstructive sleep apnea is in your future. Once accepted and treated, it becomes just another of life’s companions and not a dreaded disease.
Obstructive Sleep Apnea is a very common malady. It is familiar to many and is frequently a subject of both social and medical conversations. Individuals not engaged in frequent work with Apnea conditions may be confused by its usage and rightly so. Discussions and writings about the subject can use the term with different meanings. When used by professionals, it can also be used in various ways. It has a physiologic technical meaning; it is used as a proper name of medical conditions; and, it has a common usage that is less specific.
The word – apnea – comes from the Latin and Greek languages. The Latin ‘a + pnea’ means without breath and the Greek ‘apnoia’ means without pain. The Webster dictionary defines apnea as ”Transient cessation of respiration”. Webster’s definition fits well with the current technical use of the word, but fails to show the scope of the word’s use that has increased over the past half-century with the recognition of the associated clinical conditions.
Webster’s definition fits well with the current technical use of the word, but fails to show the scope of the word’s use…
The word is used technically to label a cessation of breathing. Sleep testing, in facilities or at home, and physiologic monitoring of hospital patients can identify periods when no air is going in or out of the nose or mouth. No breaths can be measured. These events are called Apneas.
The word is used technically to label a cessation of breathing.
The addition of chest movement measurements during these apnea events further defines these periods of apnea. If the breathing efforts are persistent during an apnea episode, the event is labeled an Obstructive Apnea. If no breathing efforts are being made by the chest, the pump that moves air in and out, the apnea is caused by the lack of chest effort and is called a Central Apnea. It is called central because breathing effort by the chest is controlled, started and adjusted, by the Central Nervous System. If the breathing problem is associated with both partially reduced chest movement and total cessation of movement, it is labeled a Mixed Apnea. As we can see, the technical apnea breathing events are further defined as obstructive, central or mixed.
‘Apnea’ is used as part of the proper name of medical conditions
‘Apnea’ is used as part of the proper name of medical conditions. These conditions were described and first recognized approximately a half-century ago, but probably have been affecting mankind for our entire history. Obstructive Sleep Apnea is the first of these. When breathing is blocked or partially blocked for 10 seconds at least five times per hour, a diagnosis of the clinical syndrome of Obstructive Sleep Apnea is established.
Central Sleep Apnea is the clinical condition where the primary form of apneas measured is central. It is established when a certain percentage of the physiologic apneas recorded on testing are the central type. Central Sleep Apnea can be the result of multiple medical issues that range from cardiovascular problems to neurologic conditions. It can be rarely seen on its own and not associated with other medical problems.
A third commonly accepted diagnostic term is Complex Sleep Apnea. This diagnostic group represents individuals with obstructive sleep apnea treated with CPAP whose breathing events do not resolve when they are treated. Their Apnea Hypopnea Index remains high. However, on repeated testing with CPAP, the breathing events are now predominantly Central Apneas. The CPAP treatment caused a change from Obstructive Apnea events to Central Apnea events. This type of medical condition is called Complex Sleep Apnea.
The term Apnea Hypopnea Index (AHI) may be new to some, but it is very important that it is understood. The ‘Apnea’ referred to is the physiologic measured Apneas. ‘Hypopnea’ is a partial obstructive breathing event measured on testing. They have the same secondary effects as apnea events but without the total cessation of airflow. The AHI is a calculated number representing the total events (Apnea and Hypopneas) per hour.
The AHI is the measurement on a diagnostic sleep test that determines if an apnea condition of some type is present. With a patient on therapy, it is the number that is followed by the physician to determine how well the therapy is working. It is measured on most CPAP machines and can be reviewed by the patient on a day-by-day basis. The AHI on a diagnostic test is and has been the measurement to determine the severity of sleep apnea conditions for many years. The AHI is an example of the technical use of the word apnea.
…the common use of the term Apnea is far less specific…
Finally, the common use of the term Apnea is far less specific than the uses we have reviewed. Often, the word is used to encompass a broad range of the field. In writings and conversations, it will be used by an author as a single word to cover all, or one, of the apnea medical conditions – obstructive sleep apnea, central sleep apnea and complex sleep apnea. When discussing Obstructive Sleep Apnea conversationally, most will speak about apnea, meaning obstructive sleep apnea. The most simple descriptive of its common use is as a substitute for the clinical conditions associated with breathing problems during sleep.
What we have covered.
1. Apnea is technically an absence of breaths (no airflow at the nose and mouth).
2. Apnea, used technically, during sleep is further defined by its features to be obstructive, central or mixed.
*Obstructive apnea
*Central apnea
*Mixed apnea
3. Apnea is used in the formal name of medical conditions including:
*Obstructive Sleep Apnea
*Central Sleep Apnea
*Complex Sleep Apnea
4. Apnea, used in its technical manner, is a component of the Apnea Hypopnea Index measurement used to judge the severity of the problem.
5. Apnea’s common use is as a general term covering one or all of the clinical conditions
“Why am I using that this thing?” they asked me. This ‘thing’ they were referring to is also known as CPAP.
Many people find themselves having had a sleep test and they are not sure why. They have a CPAP machine (Constant Positive Airway Pressure machine). Yet, they tell me, “I don’t know why.” Yes, they’ve been told they have apnea (Obstructive Sleep Apnea or OSA), but why do they need to do this? It is a question that they should be able to answer. Why do we use CPAP? Why do we treat OSA?
Why do we treat OSA?
When a sleep evaluation or sleep testing was considered for you, your physician felt it might explain some of your sleep related symptoms or medical problems. It might have been for snoring that you were not even aware had been occurring. Maybe you were sleepier than you wanted to be or more sleepy than your family or friends thought you should be. It could have been for another non-related issue. Your doctor was concerned that your problem with glaucoma, asthma or hypertension may have been made worse by or possibly even caused by a sleep condition. The test was ordered. Obstructive Sleep Apnea was found and now you have a CPAP machine.
Obstructive Sleep Apnea may cause symptoms. Excessive sleepiness, poor quality nocturnal sleep and waking up with headaches are just a few of these symptoms. Your snoring could be waking your spouse. Certainly, you would prefer not to have the symptoms. You want to sleep better and to feel better during the day.
One of the major goals of therapy for OSA, including CPAP, is to improve or eliminate symptoms. When the obstructive apnea is corrected, many of its symptoms resolve or improve, sometimes dramatically. If you had symptoms when your apnea was diagnosed, one goal of therapy is to improve or correct those symptoms.
Most symptoms of OSA are not specific.
Most symptoms of OSA are not specific. A wide range of medical conditions, some common and others not so common, can cause these symptoms. It is unfortunate, but our sleepiness or headaches do not come with labels telling us what is causing them to occur. Often, sleep apnea treated with CPAP will totally correct the obstructive events, but the symptoms that led to the evaluation and testing do not go away.
Many patients at the time they are diagnosed with significant obstructive apnea will have few or no symptoms. These individuals have varying degrees of OSA severity on their sleep testing. Surprisingly, significant OSA can be seen with minimal symptoms or even no symptoms. While the number of obstructive events per hour will generally be related to the severity of the symptoms, is it not unusual to see patients with both moderate and severe apnea with few symptoms. Even without symptoms, our current knowledge strongly supports the need for their treatment.
Many patients at the time they are diagnosed with significant obstructive apnea will have few or no symptom.
Understanding the reason for treating individuals with few or no symptoms requires a little more information. Obstructive Sleep Apnea is the repeated interruption of someone’s breathing while asleep. The obstructions result in a blood oxygen drop and an arousal to light sleep or brief awaking. These arousals are not usually associated with full awakenings. Most individuals are not aware that the obstructions have occurred.
There are two types of obstructions. The first is a total blockage of the airway with a drop in blood oxygen level while breathing efforts from the chest continues. The technical term for complete obstruction is Apnea. The second is a partial blockage of the airway while the breathing continues. These partial blockages cause the same problems as seen with an apnea. The technical term for the partial obstruction is Hypopnea. The two types of obstruction are measured during a night or portion of a night of sleep testing. The numbers of each are added together. When divided by the duration of the sleep where the measurements were made, the results represent the number during an average hour of sleep. The resulting number is the Apnea-Hypopnea Index or AHI. The AHI is the average number of apneas and hypopneas in one hour of sleep.
The AHI is considered a measurement of the severity of Obstructive Sleep Apnea. Other factors enter into the measurement of severity. The most common would be the degree of oxygen drop that occurs with these obstructive events. It is generally accepted that an AHI of less than 5 is not considered to be diagnostic of OSA. An AHI of 5 to 15 events per hour is considered mild OSA. An AHI of 15 to 30 is moderate and above 30 is severe Obstructive Sleep Apnea.
The AHI is considered a measurement of the severity of Obstructive Sleep Apnea.
In the past 40 years, thousands of research studies on Obstructive Sleep Apnea have been performed. The vast majority utilize the severity scale noted above. Those studies strongly support the current concept of the role of apnea in causing and aggravating other medical conditions.
The higher a person’s AHI on their diagnostic sleep test, the more likely they will die from a stroke or heart attack. The risk is far higher than those who have no obstructive sleep apnea. And, they die younger. When the AHI is greater than 15 per hour the risk is significant. An increased risk is measurable at an AHI of five but it is relatively small. It is very small at an AHI of less than five. It is generally accepted the long-term treatment of patients with an AHI greater than 15 at the time of diagnosis will improve secondary medical conditions and prolong life.
The second goal of therapy is obvious. It is to reduce or eliminate as many apnea and hypopnea events as possible. A person with OSA cannot know what their AHI is on any given day, night, week or month. As noted above, the symptoms do not always reflect the success of OSA treatments. However, with modern CPAP machines, technology can measure those events (AHIs) while you use the machine. Reports are now available on most machines, on most machine manufacturer’s websites, or through your physician. You and your physician can know how well your therapy is controlling your AHI.
What have we covered.
1. Obstructive Sleep Apnea can occur with minimal or no symptoms.
2. Obstructive Sleep Apnea is treated for two reasons
3. Obstructive Sleep Apnea treatment may only improve one of the reasons it is being treated.
4. The Apnea Hypopnea Index (AHI) is the number of obstruction events per hour of sleep.The AHI while on therapy demonstrate how well the therapy is controlling the Obstructive Sleep Apnea.
Three questions follow naturally from this brief review. These topics will be addressed in future post.
1. Why do I still have symptoms on treatment for OSA?
2. If I have mild OSA when diagnosed, do I need treatment?
3. What is the definition of apnea?
Why is OSA treated? The two reasons are: to improve symptoms and control the obstructive events. When we treat OSA, the treatment may be successful treating both, or just one of the two. One or both may be the reason CPAP, or another treatment, was recommended for you.
What is sleep apnea? It is an extremely common condition that should be understood by everyone. Sleep apnea is a temporary blockage or obstruction of our breathing while we sleep. A person with sleep apnea experiences repeated blockages of their air passage during sleep. The condition of obstructive sleep apnea is diagnosed when the blockages occur repeatedly.
When we sleep, our muscles relax. This can result in significant narrowing and often closure of the air passage between the lungs and the mouth and nose. The obstruction occurs between the voice box (larynx) and the nasal passage and mouth. This relaxation results in a critical narrowing. At some degree of relaxation, as the passage narrows, air has difficulty passing in and out of our lungs. A partial obstruction is called ‘hypopnea’ while a complete obstruction is an ‘apnea’. Both hypopneas and apneas have the same effects. Each is a significant obstructive event.
Figure 1
Side view of anatomy of upper airway. Top figure shows normal open airway. The bottom figure shows area of obstruction during a obstructive apnea event. The obstruction demonstrated is at the base of the tongue
Obstruction of the airway leads to physiological changes. The level of oxygen in the blood drops and the level of carbon dioxide increases. These changes occur within a few seconds. The brain, through its mechanisms to control breathing, senses these changes and immediately increases our breathing efforts. The increased breathing effort results in the opening of the air passage and the return to normal of the blood oxygen and carbon dioxide levels. This increased effort often produces a loud noise, snore or snort as airway open. The blockage will last for 15 to 20 seconds on average. An individual can wake with the choking sensation when this occurs, however, that is very unusual. Most people sleep through the entire choking episode.
Figure 2
A three minute graphic recording of a person’s normal breathing. The items recorded are chest wall movements, air movement at nose and mouth, oxygen level, snoring and sleep level.
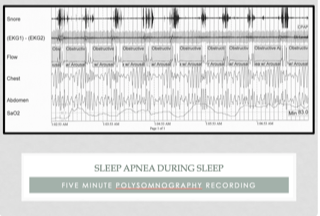
Figure 3
A three minute recording of a person having obstructive apnea events. Note the increase in chest wall movement, the absent of airflow, dropping oxygen levels, and snoring that is occurring.
The condition of obstructive sleep apnea is diagnosed when these events occur regularly and frequently. Current knowledge suggests that these have to occur at a certain frequency to create symptoms and/or medical problems. Medical professionals, insurance payers, and government bureaucrats established that five events or more per hour indicates the presence of the condition of obstructive sleep apnea.