Your interest in medicine outside of your specialty continues to surprise me. Yes, on a number of occasions I have mentioned the importance of the flow volume loop in testing lung functions. It has remained an interest of mine throughout my medical career. I am sure I can provide much more information than you want to know, as I was present at its birth for general use as a clinical test.
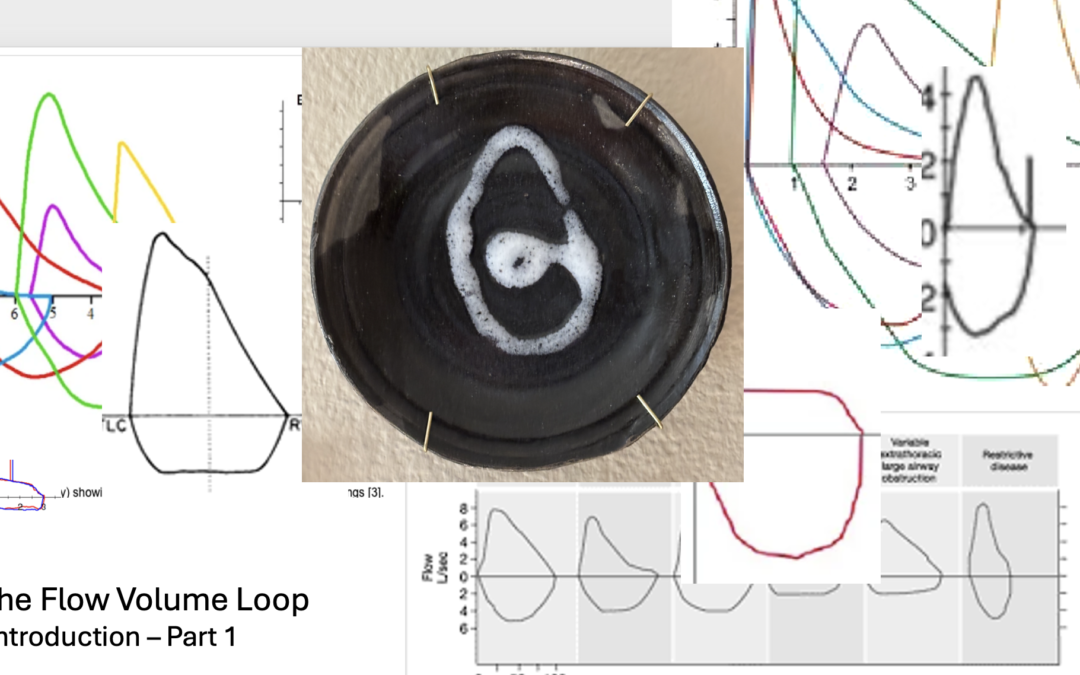
The flow volume loop is a gift to the physician. An understanding of its secrets gives the knowledgeable practitioner a world of information. It can explain or help to explain the symptoms of dyspnea and other breathing complaints. Careful review reveals more profound secrets: the unacknowledged secrets of how to understand expiratory flow, and its problems.
My love affair with the flow volume loop began in 1974 when I was made head of the pulmonary function laboratory at Walter Reed Army Medical Center. I was a newbie in the world of pulmonary physiology. Yes, I was a fully trained, knowledgeable and soon to be board certified pulmonary specialist. But the world of physiology was a whole different category of knowledge, information and details – more than any trained pulmonary physician would possess after their training in the specialty. Furthermore, I was following in the footsteps of doctors who had been more thoroughly trained in pulmonary physiology; Sidney Braman and Robert Senior, both of whom went on to extraordinary careers in academic medicine.
Drs. Hyatt and Black had just published on the value of the flow volume loop as a measurement to diagnose airflow obstructions in the trachea and larynx. The flow volume loop had not been part of our education and most patient testing facilities were not set up to make those measurements, the Walter Reed Pulmonary Testing Laboratory included. That time was before the computation of medical testing and widespread computer use in general. Flow and volume lung tests were done manually and the flow volume loop was not available to the clinician. Fortunately, or unfortunately, it is now present on almost every commercial device that measures expiratory airflow. I believe that by being so widely available, their value is being overlooked.
The technology of the 70s was evolving rapidly. Physicians were trained to understand expiratory volumes and their timing. They were also instructed in measuring basic gas changes in the blood, lung size in health and disease and the ability of gas to enter the bloodstream. These measurements were rapidly becoming common tools in the practice of clinical medicine; so too, would the new test of lung function, the flow volume loop.
Physiologists in pulmonary research had learned to measure the speed or velocity of flow with the device called a pneumotact. It provided an instant electronic signal that reflected the velocity of flowing air. Prior to that ability, volumes were measured manually and flow calculated indirectly from paper recordings. The pneumotact could be calibrated to measure the speed with which air was moving. In the 1970s this was cutting edge. Now, over 50 years later, much cheaper, more stable and reliable but similar types of devices can perform the same function and are widely available for clinical use. Almost every device currently available to measure expiratory airflow does it with some sort of electronic measurement.
The volume of air exhaled traditionally had been measured by the displacement that air would cause into a sealed container. As the air changed the position of the container, it would create a mark on paper. The inscribed marks could be physically measured and the volume of air calculated. This volume displacement was developed in the late 19th and early 20th century. In the mid 20th century, the time it took to exhale the air into the container was added as a measure of lung function. Spirometry, as it was named, had been the only pulmonary function test for measuring aspects of lung function through the 20th century and remains a mainstay of lung testing in clinical medicine today.
As a neophyte in the world of physiology, I was both frustrated and fascinated by the problems of measuring and using the flow loop. Reports by Miller and Hyatt, and then Black and Hyatt, chose to display the two parameters on an XY axis. These values needed to be measured simultaneously and plotted one verses the other. It could be projected on an oscilloscope (think of a digital screen with a line drawn on it) or on a special paper recorder. Traditionally, with spirometry testing of expiratory airflow, clinical test parameters evaluated were measurements of time on one axis and volume on the other. Those were the manually measured values. The addition of the simultaneous measurements of flow and volume, as well as the change in how they were presented, made the flow volume loop unique.
For other reasons, the lab at Walter Reed was well equipped. Previous directors had requested and received pneumotacts for use with other studies. They provided a way for me to measure the flow portion of the test. Within a few months, I was able to obtain the appropriate devices to measure volume and the special x-y recorder needed. With more than a little help from my knowledgeable staff, we created a digital signal for volume, flow, and time and then recorded them on the x-y recorder. I soon incorporated our measurement of the flow volume loop as a clinical tool. In the late 70s, subsequent upgraded testing equipment simplified these. But always in the back of my mind, those early tools brought joy to my reviews of the flow volume tests in my work.
As you can see Winston, in a relatively short period of time I was able to make the flow volume loop a clinical test available as part of the pulmonary function studies. But that was just the beginning.
Let me know if you desire more information. If you do, it may open Pandora’s flow volume box. If so, I think you would find it an interesting and valuable container.
Robert E. Hyatt MD and Black LF
Am Rev Respir Dis. 1973 Feb;107(2):191-9. doi: 10.1164/arrd.1973.107.2.191
I know it’s been a while. You haven’t heard from me in several months. Yes, I have been busy. I will try to communicate more often. First, I want you to know that all is well. Three major, well, time consuming and not ordinary events have occupied my last few months. I have completed two major projects and terminated a third.
Last summer I took extra time off from my clinical work at the Mayo. Planning ahead, I returned to it in the Fall. You will remember I was practicing part time to assist them with their backload of sleep patients. Interestingly to me, patient care is just as rewarding now as it was those years ago when I entered medicine. As they say, “You meet the nicest people.”
Computerization has ruined patient care. No, that is not exactly true. Computers have been a blessing. It is the multiple layers of regulations that are imposed through the computer programs and programmers that the doctor is burdened with completing. Large organizations are constantly modifying their systems to adjust to changing rules and regulations. I find those burdensome and onerous.
Returning to my patient care this Fall, I found it was clearly time to leave practicing clinical medicine with Mayo. My last day in September was sad but totally uneventful. So, I am officially working on my own. It is unlikely I will return to a clinical practice, but more details will follow and I will post them on the website.
“What about the other two projects?” you might wonder. They are a paper submitted and a book completed. I doubt the paper will have much success being accepted, as it is a consideration for the medical aristocracy suggesting that the AHI be modified by using total sleep time as part of the assessment for obstructive sleep apnea. I expect that I will need to offer it to another two or three journals before it is accepted for publication. Who knows, I might end up having to publish it on my own website which is certainly not the most prestigious thing to do.
And then there is the book, Reflections on Being a Physician. Depending on how I consider it, the project has lasted between three and 45 years. The book was released January 20, 2026. It is a series of essays describing the trials and tribulations I associated with becoming a physician, a series about the business of medicine from a physician’s point of view and lastly, and probably most importantly, my definition or perception of the differences between a physician and a doctor. I will send you a copy. I hope you find it an interesting read. It will be available through the website at a discounted price and available through book stores and online book retailers.
One point the book stresses is the need for doctors, physicians, nurse practitioners and physician assistants, all of us who are defined as practitioners by our government, to review and recommit ourselves yearly to our oath as a provider. It is a thought you should consider.
I will get to your other questions on my next note.
You didn’t ask for this. You probably do not even want it. Yes I know, but I promised you a primer on how to apply the qualitative and quantitative analyses of insomnia complaints. Remember, insomnia as a complaint can represent many different issues. These include difficulty going to sleep and staying asleep as well as going back to sleep after awakening or combinations of those issues. Before you can apply that information, you need a simple overview of how to consider the multiple factors that can produce difficulty with sleep.
The approach I find most helpful is based on general factors known to often cause difficulty with sleep. The categories along with a brief description are:
ENVIRONMENTAL: Environmental causes are usually recognized by the patient, but not always. Factors such as pets, spouses, lighting, thermostat settings and others are some reasons people do not sleep well.
MEDICAL: At some point almost all medical conditions may interfere with sleep. Frequent conditions are usually muscular skeletal such as injuries and arthritis. Other common, though short-term, issues include allergies and upper respiratory illnesses.
MEDICATIONS: You are not surprised to see medications, are you? Their side effects on sleep is an obsession of mine. A careful review is in order. The website has a listing under the medication tab of those and of those that frequently cause excessive sleepiness and sleeplessness.
PSYCHOLOGICAL: We all experience short term stresses and emotional upheavals that lead to anxiety and depression. Long term difficulties with insomnia can result from persistent problems with anxiety and depression. Similarly, anxiety and depression can cause difficulties with sleep. The degree of anxiety and depression needed to produce these complaints is of a magnitude that should be apparent to the patient and a perceptive doctor, though psychological issues are often difficult to assess.
HABITS: Habits can produce insomnia. Familiar to all, caffeine containing products lead the list. Less well-known dietary factors are alcohol, tea and chocolate. Not for their caffeine, but for other components. The activities a person pursues prior to sleep also can play a significant role. Food, drink, exercise, TVs and computers and lighting need reviewing.
STRUCTURE: Sleep structure refers to timing of sleep. What is the patient’s sleep duration and their time spent in bed trying to sleep? How long does the patient sleep when he sleeps well? Is the patient a night owl (likes to stay up late and wake late) or a lark (likes to go to bed early and wake early)? Are the sleep hours stable or do they change on weekends. Does the patient do shift work? How much sleep does this patient actually need? All these are factors that need to be considered.
SLEEP DISORDERS: The last category of potential issues are the disorders of sleep. Recognized disorders of sleep may produce difficulty with what a patient considers insomnia. For example, obstructive sleep apnea, thought to occur in 25% of all adults, can cause difficulty with sleep maintenance but rarely causes difficulty with initiating sleep. Restless legs and periodic limb movements need to be considered when insomnia is reported. Primary insomnia, insomnia without a known cause, is a diagnosis under this group.
Applying a qualitative and quantitative assessment allows the doctor to focus on specific areas of concern. Often, a provider will consider a patient to have primary insomnia without giving the other factors consideration. They take the patient’s complaints of insomnia – the patient’s perceptions of their sleep difficulties as insomnia – to be insomnia without a cause and proceed with medications to help induce sleep. Getting needed information from the patient is often difficult and time can limit the providers’ opportunities to explore other possible issues. For example, frequently a patient will tell me they have stopped using caffeinated products, but upon questioning, tea or energy drinks are still being used. Another major issue is medications. Patients may be on multiple medications which can produce sleeplessness or sleepiness. It can be impossible at times to separate their specific effects.Clearly identifying the details of the complaint will direct the provider to specific items to be considered for the patients diagnosis and treatment.
It is possible to identify contributing or causative factors in many patients with insomnia complaints. The qualitative and quantitative assessments often lead to specific addressable issues that can be modified or treated without the use of sleep-inducing medications. My working patterns can be summarized best in a tabular form that I have reproduced below.
When a patient’s complaints fall into one of these patterns, a more detailed history and investigation to assess that issue will follow.
And yes, Winston, I will try not to bother you with any more advice on insomnia.
RGH 29430
COMMON PATTERNS OF INSOMNIA COMPLAINTS IN SPECIFIC SLEEP PROBLEMS
Yes, that is what I said; “A problem with insomnia needs to be analyzed qualitatively.”
During my college years, I majored in the study of chemistry. The study requirements included courses in qualitative and quantitative analysis. Essentially, the study of what a substance is made of and how much of each component part is included. My comment on analyzing insomnia qualitatively means that a physician should know the components of the complaint.
The term, insomnia, has a multitude of meanings in common use as well as in medicine. The physician needs to know what the person using the term is experiencing. In essence, what are the specific issues involved? It is only with this type of clarity that the patient’s situation can be assessed. The analysis includes the effects on daytime activities and is designed for nocturnal sleepers. Those whose primary sleeping time is during the day, for example shift workers, require a different approach.
Difficulty falling asleep or initiating sleep is the most recognized problem described by the term. Defining the time required for sleep onset is the first step in assessing insomnia. A problem with sleep initiation may be someone’s sole issue or it may be just one part of the patient’s problem.
Another difficulty often described as insomnia is waking frequently during the sleep period. It is common and considered normal to wake once or twice a night. Waking more often disrupts sleep and is frequently an issue for the patient. Those with this complaint may or may not have a third type of problem, returning to sleep.
Returning to sleep after waking during your night of sleep, can be a singular issue or can be associated with other insomnia issues. Some will wake frequently while others will wake only once or twice. A problem returning to sleep can occur in either situation.
Waking earlier than desired is another issue commonly reported as insomnia. All of these complaints may occur independently or in combination with one or more of the others.
Knowledge of the effects of the sleep problem on daytime wakefulness and napping is helpful diagnostically. Is the person sleepy during the day? Do they nap? Do they nod off?
To analyze complaints of insomnia, a physician needs to understand:
Are there problems with sleep initiation?
Are there problems with sleep maintenance?
Are there problems with returning to sleep after awaking?
Are there problems with waking too early for the day?
Are there problems with daytime sleepiness?
A patient’s historical ‘insomnia qualitative profile’ information is required for accurate assessment. Unfortunately, getting the information can be difficult, time consuming and even impossible. When obtainable, it will help with establishing a diagnosis, but a pattern of difficulty does not indicate a specific reason or cause for the issues. In fact, many or most individuals will have more than one potential causative or aggravating issue.
The frequency the symptoms occur and their intensity are important in narrowing the potential reasons or contributing factors to the sleeplessness problem. How significant is each of the symptoms reported? This step is the quantitative analysis of each of these factors
Diagnostic considerations of insomnia require knowledge of the specific complaints (the qualitative analysis) and the degree to which they are present (the quantitative analysis) for assessing factors that are known to produce insomnia.
So Winston, I have returned to my youth of qualitative and quantitative analysis. A famous troubadour once penned a song; “All my life’s a circle, sunrise to sunset.” So it appears to be. I suspect this is more than you probably wanted to know. Maybe I should prepare a short primer for you on the roles of the qualitative and quantitative assessments in identifying the factors, conditions and behaviors known to produce and aggravate insomnia.
Once I lost a hammer. It was a tool I earned in my youth while working to finance my education. It taught me to respect the tools I use in my work. On a past occasion (30 years ago), I wrote how doctors should view their tools: a major one being hospitals. My hope was that practicing doctors would work to influence those institutions for the better. Oh, such were the dreams of my youth. Hospitals are now conglomerates operated by boards and individuals steeped in the profit motives common to all corporations. These are boards and individuals who are far removed from our Oath. They are focusing on the growth and profit for the corporate owners, not on a profit to benefit the community, patients, employees, operations and doctors that it serves. It is a tool that I believe is lost for the lifetime of most current doctors. Now a newer tool already widely used is my current concern: the electronic medical record.
This story begins with my Apple IIe. No, it actually begins much earlier than that. It begins my senior year in high school. An opening in my class schedule allowed me to choose a class of my choice. I chose typing. As a result, I had the advantage of being able to type in college, medical school and even now. My time in high school was before electric typewriters and computers. Since I could type, buying my IIe let me explore the world of computing. It was great fun and allowed me to explore simple basic programing, even writing a program for the interpretation of blood gas test results. Within a short time, professional programers were producing much more sophisticated versions. My skills were in the medical, not the computer field. I need not burden you with the progress in the computer world.
As my medical practice matured, my use of computers kept up with their ability to make life easier. My specialty practice needed quality reports to keep its referring physicians informed as did my work interpreting hospital studies. The computers of the 90’s and since, allow for the creation of these. More ominously, the financial aspects of medical practices began to require computerization. Progress in technology and increased control over fees and payments by outside businesses and government required more and more computerization. Then, a little more than a decade ago, the electronic medical record appeared. It first was a way to organize the doctor’s medical files, but integration with the financial aspects of practice rapidly followed. The electric, digital medical record was born. Hospital and medical practices, with significant government encouragement, widely adopted the electronic system. Use became mandatory for some.
“Open the Pod Bay doors, Hal.” Requested astronaut Dave Bowman.
“I’m sorry, Dave. I’m afraid I can’t do that.” Responded Hal, the 9000 Computer
“The X system does not allow that. I think you can work around it. You will need to go to the ‘order’ tab, then the ‘misc’ tab. That will get the dropdown menu for other items. It is probably listed there.” The support staff cheerily reviewed for me. Their acceptance of the complexities of the digital medical record is probably based upon their knowledge of its inner working. Most of the staff were born after my IIe was manufactured. Raised with and around computers, their acceptance of these difficulties is as understandable as it is disturbing. Though their followup comment indicates dependency on a higher authority, “Sharon, Medical Record X’s representative, can probably help us with that. I will reach out to her. I can have something for you in a few days.” This interaction has become more and more common when a doctor working for a large group or organization runs into issues with documenting, placing orders or communicating with their patients.
Don’t misunderstand me. They are trying to be helpful. They definitely know more about the X electronic medical record than the physicians do. What is irritating is their acceptance that it is the holy grail of records. Their entire lives have been during the computer age. It leads them to accept all its faults and I suspect, to not fully understand why just a few more clicks to memorize and perform does not leave me happy. What happens when the business Medical Record X changes the clicks, deletes the item or task needed or I forget the clicks? I am back to square one.
“Dave, this conversation can serve no purpose any more. Goodbye,” concludes Hal when it tires of discussing opening the pod bay doors with Dave. Hal has made a decision and it will not change. Dave will be left in space. Dave using human ingenuity ultimately finds an alternate way back into the space craft.
Recently it was announced, company X had added an upgrade that some of the support staff were using. It is a program to change a prepared patient message to a calmer more comforting tone and words. We were told it has helped improve the patient’s perception of a few of the staff messages where it has been used. How does it work? A message is prepared. You ask the program to review it. It does, and then changes how the message is phrased and addressed the patient. Red flags flew in my head. Is it the first step in eliminating the human contact in medical care? For example, just feed the result of a test to the system and it prepares and sends the message. Will it become similar to the multitude of robo calls, messages and commercial computer chats to which we are now exposed? Yes, I am being a bit paranoid. At the least, it does indicate some of the support staff need to improve their communication skills.
“Just what do you think you’re doing, Dave?” Hal asks.
“Dave, stop. Stop, will you? Stop, Dave. Will you stop Dave? Stop. Dave.” Hal attempting to stop Dave from deactivating it.
Hal’s finial vocalizations, “I’m afraid. I’m afraid. Dave. Dave my mind is going. I can feel it. I can feel it. My mind is going.”
Dave completed his mission without Hal. Following Dave’s guidance, maybe we need to disable X. No, that would be like doing away with the car, a terrible thought. Without the automobile, modern society would crumble. There are cars made to go 180 miles per hour and travel through deserts and mountains with ruts for roads, but few will purchase them and even fewer use those features. Unfortunately, the typical electronic medical record system comes with the 180 mile per hour and off-road options. Unlike the car of your choice, you are more a passenger than the driver of the record.
Those options on the electronic record are controls that constrain the medical practice to conform to insurance and government standards. We should recognize the dangers of its controlling nature. It is very similar to government. Governments have an essential role in allowing a free society to flourish and too much government results in tyrannical control. In our era, China, North Korea, Cuba and Russia are good examples of too much control. The computer has an important, almost essential role in medicine, but when controlled by self-interested parties, it can become tyrannical.
As the ultimate users, doctors, and maybe patients, need to police the features included in the computerization of the medical record. Let’s not buy those controlling features. Remember, your role in most systems will be that of passenger, not driver, and it is going to be a long, frustrating, expensive ride.
*From “2001, A Space Odyssey,” a movie by Stanley Kubrick released in 1968 to mixed reviews. Now considered one of the greatest and most influential films ever made. These quotes are taken from a section of the movie on a space voyage from Earth to Jupiter where Hal, the human like computer controlling the flight and the space craft, has locked the human astronaut out of the space craft and refuses to let him back in. You see, Hal had made a mistake and could not admit it. How very human like.
Yes, yes, Winston, I have heard about the new medication approved by the FDA. It has been heralded as the first drug approved for the treatment of Obstructive Sleep Apnea. “Is it so?” you ask. It is, but as an infamous man once said, “It all depends on what the definition of is, is.”
The approval is the FDA giving it an indication for use in obese patients with moderate to severe obstructive sleep apnea. With that approval, it becomes the first medication to have an indication for use in Obstructive Sleep Apnea. This is the fact that has been in multiple news outlets and led to many questions of sleep doctors by our patients. It is important to know more about the details.
The approval followed a multi-million dollar, manufacture sponsored study that was published in the New England Journal of Medicine (NEJM). The study focused on using the weight loss drug in obese individuals with Obstructive Sleep Apnea. Unsurprisingly, the weight loss induced by the medication resulted in improvement in the apnea condition. The treated patients were compared to those treated by diet alone who lost little weight during the study. It was not compared to other weight loss drugs. The article received wide acclaim and attention.
What was known about excessive body weight, weight loss and Obstructive Sleep Apnea before this study? I have an interest in the subject and have followed the work in the field since seeing my first patient with sleep apnea while serving in the Army. He was thin as a rail, by the way. Current knowledge is that we know slightly more than half of all newly diagnosed apnea patients have problems with their weight. We know that of those patients who experience significant weight loss, apnea is eliminated in 18-20% of the obese patients. The others are usually improved, but apnea is not eliminated.
My review of the NEJM article can be summarized briefly. The drug causes weight loss (previously known) and the weight loss improved apnea in many with it. Does it work any better than weight loss by any other means: diet, counseling or other weight loss drugs? Who knows? The study does not address the issue. Does it improve apnea over and above the effect of losing weight? Who knows? The study does not address the issue.
What did the article do? I don’t think it provided any new information. It most likely – I speculate here – influenced the FDA to add the Sleep Apnea with obesity indication to the medication’s approved usage. I suspect that the several million dollars spent for the study resulted in far more notoriety and media attention than any amount of advertising money could buy. Additional facts for you to consider are the cost of the medication and the duration of treatment it requires. A quick Internet search shows it to cost between 900 and 1,000 dollars a month on a well-known discount site. The duration of treatment is potentially life long.
No Winston, it is not proven to be a drug for apnea: just another very expensive drug for weight loss.
I am sorry to go on like this Winston, but let’s face it; we are all concerned with our image. It is a basic human trait. Doctors are not immune. When I last wrote, my feelings were running high regarding the reports all doctors are responsible for completing. I stressed the importance of topic or idea segmentation to improve communication, but good communication requires much more.
All reports need more than just the appropriate formatting. What do we include? Of course the type of report dictates its contents. Test interpretation results, by their nature, report the data generated. Hopefully, these are skillfully separated into pertinent presentations or discussions of individual parameters. For the tests performed, a summation of the results should follow with any appropriate, suggested next steps.
Most medical reports are the results of our direct interaction with patients. Histories, physicals, consultations, progress notes, surgical reports and summaries of clinical notes are examples. While these reports are segmented in a long defined manner, they are often subject to abuses of several easily identifiable types.
The segmentation of doctors’ reports summarizing patient interactions is over 50 years old. New physicians are trained to segment their reports. Traditionally, such reports are divided into the chief complaint, history of the present illness, past medical history, medications, allergies, system review, physical examination, available test data, analysis, impression of the potential diagnosis and the plan for the patient’s future. It seems a lot, and it is, but it is what we do. A great deal must be accomplished in the time we allocate to meet with the patient.
Changes in the notes documenting patient interactions have been suggested in the past few decades; most notably the problem oriented segmentation of such reports. Segmenting reports to specific problems has been suggested to improve the identification and analysis of each problem. These approaches have has varying degrees of acceptance and have definitely improved communications of information. But abuses creating reports continue.
In reports, the all-encompassing segment on analysis is too frequently a single paragraph where the facts of the case are reviewed, an appropriate diagnosis assessed and recommendations presented. When prepared by a thorough physician, this portion of the report will be subdivided as appropriate for the facts of the case to discuss each individual item. The specific recommendations will be provided separately.
There are common techniques used in creating these reports that stand out as inappropriate when overused. I refer to the users of these techniques as the ‘filler’, the ‘ black and white,’ and the ‘obfuscator.’
A ‘filler’ delights in computer generated reports. At the appropriate place in his report, the ‘filler’ will copy and paste entire test results, consults, radiology or laboratory reports into their own. Another common filler technique is to insert a computer generated medical list completed by a nurse or assistant that is so easy to do and so official looking. All the while, to the educated eye, the presentation is screaming that they couldn’t identify what was important from the inserted report so they just included it all in their own. You can almost hear them say, “Look at my impressive comprehensive report.” Certainly the lengths of the reports are impressive. I recently received a consultation on one of my patients where the doctor used the filler technique to the maximum. The dictated computer report was 16 pages long.
The person using the ‘black and white’ approach is the binary report creator: lots of data and no nuances. The ‘black and white’s’ history will include yes and no answers for symptoms, give number results for standard questionnaires and closely follow current medical guidelines. This is particularly true for any therapeutic recommendations on the reports.
The ‘obfuscator’ will fill their assessments with facts and lengthy discussions of potential diseases and conditions, while not providing a consensus on issues of concern to the patient. Could it be they do not have an opinion, do not have a clue or just do not want to express an assessment of the patient’s issues? Maybe it is a “look how smart I am” assessment.
All of us use these techniques to some degree in our reports. Most medical reports tend to be repetitious and dull, but like a story, they can benefit from a logical progression in the presentation and understandable writing. Brevity, to a point, leads to clarity of communication.
I am sorry to go on like this Winston, but let’s face it; we are all concerned with our image. It is a basic human trait. Doctors are not immune. When I last wrote, my feelings were running high regarding the reports all doctors are responsible for completing. I stressed the importance of topic or idea segmentation to improve communication, but good communication requires much more.
All reports need more than just the appropriate formatting. What do we include? Of course the type of report dictates its contents. Test interpretation results, by their nature, report the data generated. Hopefully, these are skillfully separated into pertinent presentations or discussions of individual parameters. For the tests performed, a summation of the results should follow with any appropriate, suggested next steps.
Most medical reports are the results of our direct interaction with patients. Histories, physicals, consultations, progress notes, surgical reports and summaries of clinical notes are examples. While these reports are segmented in a long defined manner, they are often subject to abuses of several easily identifiable types.
The segmentation of doctors’ reports summarizing patient interactions is over 50 years old. New physicians are trained to segment their reports. Traditionally, such reports are divided into the chief complaint, history of the present illness, past medical history, medications, allergies, system review, physical examination, available test data, analysis, impression of the potential diagnosis and the plan for the patient’s future. It seems a lot, and it is, but it is what we do. A great deal must be accomplished in the time we allocate to meet with the patient.
Changes in the notes documenting patient interactions have been suggested in the past few decades; most notably the problem oriented segmentation of such reports. Segmenting reports to specific problems has been suggested to improve the identification and analysis of each problem. These approaches have has varying degrees of acceptance and have definitely improved communications of information. But abuses creating reports continue.
In reports, the all-encompassing segment on analysis is too frequently a single paragraph where the facts of the case are reviewed, an appropriate diagnosis assessed and recommendations presented. When prepared by a thorough physician, this portion of the report will be subdivided as appropriate for the facts of the case to discuss each individual item. The specific recommendations will be provided separately.
There are common techniques used in creating these reports that stand out as inappropriate when overused. I refer to the users of these techniques as the ‘filler’, the ‘ black and white,’ and the ‘obfuscator.’
A ‘filler’ delights in computer generated reports. At the appropriate place in his report, the ‘filler’ will copy and paste entire test results, consults, radiology or laboratory reports into their own. Another common filler technique is to insert a computer generated medical list completed by a nurse or assistant that is so easy to do and so official looking. All the while, to the educated eye, the presentation is screaming that they couldn’t identify what was important from the inserted report so they just included it all in their own. You can almost hear them say, “Look at my impressive comprehensive report.” Certainly the lengths of the reports are impressive. I recently received a consultation on one of my patients where the doctor used the filler technique to the maximum. The dictated computer report was 16 pages long.
The person using the ‘black and white’ approach is the binary report creator: lots of data and no nuances. The ‘black and white’s’ history will include yes and no answers for symptoms, give number results for standard questionnaires and closely follow current medical guidelines. This is particularly true for any therapeutic recommendations on the reports.
The ‘obfuscator’ will fill their assessments with facts and lengthy discussions of potential diseases and conditions, while not providing a consensus on issues of concern to the patient. Could it be they do not have an opinion, do not have a clue or just do not want to express an assessment of the patient’s issues? Maybe it is a “look how smart I am” assessment.
All of us use these techniques to some degree in our reports. Most medical reports tend to be repetitious and dull, but like a story, they can benefit from a logical progression in the presentation and understandable writing. Brevity, to a point, leads to clarity of communication.
Yes Winston, I am very opinionated about writing medical reports. Any document in medicine has a purpose for being created. Those purposes have evolved as well as the manner in which the information is generated. The types of reports have multiplied. My obsession with the creation of reports occurred as a result of a coping mechanism during my career’s evolution.
Once trained as a medical doctor, I was slow to make a decision on what to do with my career. My basic introduction to medicine had, by my own choice, been one of exposing myself to multiple fields. Once I selected internal medicine, it was shortly thereafter that I decided to concentrate my work in the field of lung diseases. With good fortune, ambition and fate, a short five years later I found myself in charge of the Pulmonary Function Laboratory at Walter Reed Army Medical Center.
My post graduate medical training at county, university, veteran and military institutions was designed to train me to be a medical doctor in the specialty of lung diseases. My knowledge of physiology was good for a pulmonologist, but almost superficial for my added job responsibilities. I set a goal to learn the field at a deeper level and was able to progress greatly over the years while I held that position.
On the practical side, tests were being done daily. Doctors from numerous specialties and clinics were ordering tests of lung functions and a report had to be generated for each. It was my responsibility to oversee the creation and quality of a large number of those reports. After leaving the military, I had similar responsibilities at a cardio-pulmonary specialty hospital for an additional 16 years. During the following 20 years, my reports were limited to interpreting sleep tests. Throughout my career, I have been responsible for an extremely large number of medical test reports.
In those early years I was progressively learning more about the details of my work. In my training and previous experience, I was exposed to reports which consisted of consolidated paragraphs with a signature at the end. As I learned more about the physiological aspects of our studies, I would segment portions of my reports to review each one in more detail. Over time, my reports became multiple, small descriptive paragraphs with many sections. At the end, I would summarize the results briefly.
As my knowledge increased, the report format evolved. I was separately analyzing and reporting each group of measured parameters. By doing so, their relationships were clearer and abnormal parameters were more readily identified. Constructing the report by simply separating each parameter analyzed, insured that the interpreting physician reviewed all the parameters and improved the communication of important results to the requesting physician.
Now, after 50 years working in this field, I am struck by how many respected doctors and physicians do not use such a format. Their single paragraph reports appear congested and chaotic when read, making it difficult to identify important numbers and features.
And yes Winston, our clinical reports, consults, progress notes and similar communications benefit from clear thinking and organization. It does not matter if the report is for other physicians, for your future reference, for insurance review or for the patients; a compartmental organized report demonstrates a thorough analytical analysis.
A medical report is a window on the organization and thinking of the professional who prepares it. A segmented, organized report communicates better and ensures attention is paid to each aspect of the subject. Continuous paragraphs of summarized facts suggest a chaotic, unorganized mind.
Yes, I am aware of the national TV ads for the hypoglossal nerve stimulator for Obstructive Sleep Apnea. Earlier this year I prepared an information sheet on the subject. I will add it to this letter.
It is a second line therapy and works for a limited sub group of patients with Obstructive Sleep Apnea. CPAP is far more successful in controlling sleep apnea.
It primarily indicated for those who have failed CPAP. Unfortunately, there is no accepted definition what constitutes failing CPAP therapy. Reasons for stopping CPAP are many and sometimes complex. I have been intrigued by the issues that cause a patient to discontinue or be unable to use it and will add more on the subject on another occasion.
RGH 29.112 Sept 2023
Hypoglossal Nerve Stimulator (Inspire) May 2023
Device
“Inspire” is a device that senses an obstructive apneas and then sends a signal to the hypoglossal nerve through a wire. It activates the nerve, which causes the base of the tongue to move forward. The device, wires that sense the apnea and the wire from the device to the nerve are implanted under the skin. It is remotely controlled.
Candidates / Indications (Varies from FDA, Insurance and Medical societies)
Its primary indication for use is failure to be able to use CPAP. Problems with insomnia, restless legs or other sleep disorders must be controlled before being considered for Inspire. The obstructive apnea rating (apnea hypopnea index or AHI) on diagnostic testing should be between 15 and 65. Weight should be a BMI of under 32. BMI varies by height. For a 5’11” person a BMI of 32 is 225 lbs. Some insurances will allow a slightly higher BMIs. You must be older than 18 years of age. It is indicated when apnea obstruction occurs at the base of the tongue.
Cost
A rough estimate of the cost of the device, its implantation, testing and physician visits will be between forty and fifty thousand dollars.
Insurance Coverage
“Inspire” is a second line therapy and insurance companies only approve those who have failed other forms of treatment.
Process
If you meet the criteria for the device, you will be evaluated to see if the device will correct your apnea. The evaluation steps include a facility based sleep study, a sedated endoscopy of your upper airway and provider visits. Many will not fit the type of obstruction that the device will correct and will not be candidates.
If you are a candidate, then implantation, physician review and repeat testing to insure appropriate function will be required. These steps include surgery, a post activation facility based sleep study and provider visits.
The overall time from initial consideration to successful activation is about 5 to 6 months. Medical follow up currently is recommended every 6 to 12 months.
Results After Implantation
The goals of treating obstructive apnea are to reduce the AHI to less than 5 and to improve the quality of sleep. CPAP will achieve AHIs < 5 a very high percentage of the time. The Inspire device will reduce the AHI to less than 5 in approximately 50% of recipients. The rest will have a reduction in their AHIs but not to normal levels. Standard therapies such as CPAP may still be needed.
Other Considerations
“Inspire” is a man-made product with batteries. Wires can break. Wires cannot easily be removed. Batteries or new wires may be required in the future. There are a limited number of experienced physicians available to deal with the device. Other devices may still be needed and recommended to control your apnea condition.
It is inspiring to learn of your interest in sleep apnea. I will be happy to do my best to simplify, clarify and muddy your understanding of the AHI. AHI stands for Apnea Hypopnea Index. It is the standard for defining the presence of significant sleep disordered breathing and the condition of Obstructive Sleep Apnea.
It started long ago in the history of sleep medicine. In actual time, it was just 40-50 years ago. Physicians noted breathing problems during sleep. Over a decade or so it was clear from investigations that the problem was one of blockage of the airway in the throat during sleep. The blockage resulted in less air getting in and out of the lungs. The blood oxygen levels would drop, while the carbon dioxide level would increase. The sleeper responded with increased breathing efforts, which opened the airway. By the 1980’s, testing for these variables had evolved from investigative to the clinical practice level.
The AHI is the fundamental measurement for obstructive and central types of sleep disordered breathing. The A stands for apnea, or absence of breath. The H stands for hypopnea, or a critical reduction of airflow causing the same physiologic changes that the apnea produces. The I stands for index but actually represents a measurement of rate, the number of apneas and hypopneas per hour of sleep. The apnea as used in AHI represents the absences of air movement at the nose and mouth. Respiratory efforts by the diaphragm and chest may or may not be present. These are the simple definitions.
Clinicians and physiologists have much more specific definitions. Our definitions include the magnitude and duration of physiologic changes, as well as the types of equipment used for the measurements and the frequency of the changes. It should not surprise you that significant debate continues about the details of those changes. Opinions differ. Unfortunately, the efficient computerized testing systems we utilize, ease the burden of testing large numbers of people, but limit the ability to look at multiple variations of potential changes in definitions.
In this country, current technical definitions and the threshold for diagnosing the medical condition of apnea are cemented in place by the regulatory bodies; Medicare and commercial insurance companies set the standards. While the definitions set are supported by reported evidence, the standards are far from perfect and will not change soon.
The AHI is the gold standard for the definition of obstructive and central sleep apnea. Five events, apneas and or hypopneas, per hour of sleep meet diagnostic level for apnea. The level of 5 events was arrived at arbitrarily, based on early work in the field. Although accepted by those regulating groups, the actual minimal AHI needed to establish the diagnosis is not really known.
It is known that the higher the AHI the greater the risk for long-term medical problems. When a sleep study is complete and the AHI criteria for apnea is met, it is described as mild (5-15 events}, moderate (15-30 events) or severe (>30 events) apnea. The adjectives (mild, moderate and severe) represent the long-term risk for medical complications, not how a person feels. These separations into different severities of apnea, represent more tradition than science. In fact, the AHI is only a good predictor of severity for long-term complications at high levels (more complications) and very low levels (less complications). In the decades since these definitions for the onset and the severity of the disease were adopted, much research has been done. It appears that further definitions of these obstructive events would improve the accuracy of our diagnoses and the predictability of the future for the patient.
The current definitions have served time well. As a clinical tool, the AHI has proven to be extremely useful. It is accepted worldwide. Tremendous improvement in diagnosis and therapy for sleep apnea has occurred utilizing these measurements. There are limitations, however. This is specifically true when scientific studies of the condition are performed.
The role of low oxygen levels has been investigated more than any other factor. You will recall oxygen is measured on testing by the noninvasive transcutaneous method that reports oxygen saturations. Our technical definitions include a certain drop in oxygen saturation that is caused by the interruption to the airflow during the breathing events. The roles of the duration, severity and timing of the drop of oxygen in the sleep pattern as well as the total time spent at certain levels of oxygen desaturation are not known. Studies reviewing low oxygen levels during apnea suggest that the time spent with saturations of less than 90% together with the AHI is more accurate in predicting long-term medical complications than the AHI alone.
Another major factor not addressed with current testing is the use of a rate measurement for diagnostic purposes. A rate does not measure total exposure to apnea events. That is dependent on actual sleep time. An easy example is the difference of someone sleeping six hours versus another person who sleeps nine hours. They both can have the same AHI, but the person sleeping nine hours will be exposed to 50% more apnea events than the person who only sleeps six. The importance of exposure has not been studied at all.
The events we measure, apneas and hypopneas, do not occur uniformly throughout a night of sleep. The event frequency can change based upon body position. They can occur more while sleeping on the back verses the stomach. The events can occur more in REM sleep than in slow wave or Non-REM sleep. Research into the effects of these variables as predictors of long-term outcomes is limited.
Well, I believe it is time to close. The AHI is an immensely useful tool in the diagnosis and treatment of sleep apnea. It is the gold standard measurement for the diagnosis of sleep apnea. It needs to be improved upon and will be. As you will learn throughout your career, medicine changes slowly. Opinions are more rigid in medicine and in science than most believe. So, keep an open mind. This, like all things medical, will change with time.
Yes, I will try to answer your question. I understand your training has led you to believe that healthcare is a right. Why, you ask, did I pause before saying, “It’s not that simple. But if it were, the answer would have to be no.”
Consider first what is meant by the term, healthcare. Like most words, it is likely interpreted differently by almost everyone. The views will run from having clean water, a family doctor available for medical problems to those that would include anything to do with a person’s health. These are widely divergent categories of products and services based on different delivery systems and business models. It is almost impossible to discuss a ‘right to healthcare’ without understanding everything that is included in the discussion – the components of healthcare.
It is not the only term that needs to be defined. What do the promoters mean by the word, right? Maybe it is best to consider its meaning first.
When right is used as a noun, as it is in a ‘right to healthcare,’ common definitions according to Merriam-Webster include: qualities of moral correctness or moral propriety; something to which someone has a just claim; something to which someone may claim as their due; and, a cause of truth or justness. The proponents of a ‘right to healthcare’ usually mean the second or third of these definitions, a just claim or their due.
Healthcare has only one definition listed. Merriam-Webster defines it as ‘efforts to maintain or restore physical, mental or emotional well-being especially by trained or licensed professionals.’ Practically speaking, this definition would essentially cover all aspects of personal and public health. It would include the fields of preventive medicine, public health and personal medical care along with institutional medical care. Each of these fields is unique in how it is currently organized and delivered while sharing some common features. The shared features include the need for physical plants of operation, equipment to provide the services, support staff to carry out the services and a professional staff. These factors are needed in varying quantities and of different types for each of these fields of endeavors.
For clearer understanding we need to look more specifically at the services included in healthcare. These would include public health services, preventive medicine services (public or individual), individual’s urgent and chronic medical care, and institutional care (hospitalization and similar). We need to consider all the services that might be determined to be healthcare.
Public health is widely practiced throughout most local communities in our country. Public health services maintain and ensure clean water and adequate sewers, track communicable diseases and advise the population about those diseases. Their services, physical plant, equipment, staff and professionals are paid for and employed by government units. They are paid for by taxes and by fees for water and sewer services. For the majority of urban areas in this country, these health services are for all practical purposes already a right provided by the government. Certainly, there are exceptions for rural and smaller communities, but most citizens already enjoy public health as a government service. Paid for by their taxes.
Preventive medical services are currently provided by both government operations and individual medical providers. Examples of government services include monitoring of new and current medications for problems, providing recommendations for vaccinations, and monitoring of medical devices. Again, the facilities, staff, equipment and professionals are supplied and paid for by the government taxes and fees usually paid by the businesses for the service.
At a more personal level, physicians, providers, healthcare businesses and employers (insurance companies, medical practices, clinics, hospitals and businesses) may provide guidance and assistance on preventive medical measures that an individual needs. These businesses provide the physical plant, staff, equipment and professional organization needed. The expense for these services is recouped through fees, insurance payment, employers and other methods. The healthcare provided at this level is the first at which an individual may be responsible for all or part of the cost of the services.
The next component leads further into individual responsibility, providing an individual’s urgent and ongoing medical care. This is the form of healthcare we are familiar with and what is most often thought of when discussing ‘a right to healthcare’. In our country’s history, these services have been provided by individual professionals who own and operate their own businesses. Recent change in economics, economic policy and legal structures of medical businesses has led to more large organizations (hospitals and insurance companies) owning more of these types of businesses. In these operations in any form, the expenses – from cotton swabs to physician income – are paid for by individuals, either directly or through surrogates (employers, insurances or others).
An individual’s surrogates are the primary payees for the institutional care portion of our healthcare delivery system. This portion of healthcare, hospitalization primarily, is where the largest cost (facilities, equipment, staff and professionals) occurs. Again, most of the cost is paid for by individuals or their surrogates.
In these areas of healthcare where the individual is mostly responsible for the cost of the service, there is one major group of individuals that is not responsible directly. Those are individuals on government insurance such as Medicare. In Medicare and other government plans, a person may have a markedly reduced or no exposure to the direct cost of the services. Those who argue for a ‘right to healthcare” would like all services for all citizens to be paid for by the government.
My comments have gone on long enough so I will save my additional thoughts for a future letter. I would add in closing what I think summarizes the whole question.
A ‘right to healthcare’ should mean everyone has access to and freedom to decide how to obtain their healthcare. At present, I would argue that it is already the case, but it is disappearing rapidly. In reality, the discussion is not about freedom to get healthcare, but getting healthcare for free.
There are complex airway dynamics resulting in blockage of the upper airway producing Obstructive Sleep Apnea. Although complex, the process can be viewed in a general non-technical manner to help one understand the causes of obstructive sleep apnea.
In such an overview, we find two components to the events producing blockage of the airway during sleep: airway muscle relaxation and airway size. How does each of these contribute to the development of obstructive apnea?
The basic event of sleep apnea is the relaxation of the upper airway (the throat above the Adam’s apple to the nose and mouth) narrowing it critically or totally, resulting in a blockage limiting the amount of air traveling into or out of the lungs. This causes a drop in the blood oxygen and an increase in the blood carbon dioxide. These are changes, which the brain notices immediately. The very next breathing effort by the diaphragm is stronger. These efforts keep increasing until two or three breaths later, on average about 15 to 20 seconds, the effort is strong enough that the throat opens and air moves in and out again. Commonly, but certainly not always, this is accompanied by a loud snore or snort. These events are what produce Obstructive Sleep Apnea.
While these events alone may not be medically important, they produce problems when they occur repeatedly. A measurement of five events per hour while sleeping is considered diagnostic of Obstructive Sleep Apnea in the United States. Problems are thought to develop at this point.
Relaxation of the tongue and pharyngeal muscles play a role in developing these events. As we age, muscle tone decreases. Strength reduces. Tissue tone becomes slack, to say the least. We have all seen the effects of age in our family, friends and maybe even ourselves. The same changes take place in our tongue, pharyngeal muscles and supporting tissues. The prevalence data for obstructive sleep apnea show a steady increase with age. Those greater than 70 years of age are reported to have an 80% frequency of occurrence.
Muscle relaxation and muscle changes with age are major components of the causation of obstructive apnea.
What role does airway size play in causing obstructive apnea? The size of the airway determines how much muscle relaxation is needed for the critical narrowing to occur. Smaller airways will close more easily than larger ones
It is best to look at the airway size as two issues – weight and genetics.
In the 1960s, doctors discovered and described the obstructive apnea problem in obese patients. For the first 20 years after its description, many strongly believed that obstructive apnea was just a complication of obesity, not an independent problem. When a person gains weight, the fat tissue is added over the muscles below the skin in most areas of the body, including under the skin in the throat. The accumulation in the throat makes the size of the airway smaller. With a smaller airway, less relaxation is required to cause the critical narrowing resulting in an obstructive apnea event.
It is now well known that at certain weights almost everyone will have apnea. The medical community uses a measurement that is a calculation based on height and weight. This is called the Body Mass Index or BMI. A normal BMI is 20 to 25. When a person’s BMI reaches 40, ninety percent of those individuals will have sleep apnea.
Obesity can cause sleep apnea. What is its contribution to all those individuals with the condition? No one agrees and there has been ongoing debate since the 1970s.
Like most medical controversies, variation in the reported studies makes the issue more difficult to understand.
Early attempts to understand the effects of weight loss on apnea used an improvement in symptoms as the mark of correcting the problem. When obese patients with apnea lose a significant amount of weight, they feel and sleep better. The authors of those reports concluded that obstructive sleep apnea was cured by weight loss. But, did it really cure the apnea?
As more studies were done, the investigators began testing for apnea after weight loss. To assess the effect of weight loss on correcting apnea, the reports used changes in patients’ sleep test measurements. Typically, they would use a percentage drop in the number of apnea events or select a set level of events at 15 or 5 per hour. The level of 5 is the diagnostic level accepted for the diagnosis of the condition. These studies report a high level of symptomatic improvement with weight loss. Unfortunately, only 10-15% of obese patients will drop their levels below 5 after weight loss. Most will reduce the number of events limiting the severity, but few can be considered as cured. For an individual, weight loss can have significant beneficial effects on treatment, need for treatment and symptoms. However, when viewed as a cause, few can be considered to have obstructive apnea caused by obesity.
My experience reported a few years ago at a community sleep center gives an insight. For every one hundred cases of newly diagnosed obstructive sleep apnea, 60 will have BMIs in the obese range, meaning that 60% were obese. After weight loss, we know only 10 to 15% of individuals will have their apnea event drop below 5 per hour. In the one hundred newly diagnosed individuals with apnea, weight loss will correct the apnea in only 6-10 of the 60 who had weight issues. The other 50- 54 previously obese now are of normal weight and still have apnea. They will feel better after weight loss, but they will still have apnea. There are now a total of approximately 90 who still have apnea. Why?
There is the problem of muscle relaxation of course, but there is the other component of airway size – Genetics.
Sleep doctors look at throats when evaluating their patients. As a practitioner for many years, I have looked at the throats of thousands of patients with obstructive apnea. How many abnormal throats have I observed? Not many. I have seen one throat malignancy in my last two thousand exams. By including enlarged tonsils and changes due to prior surgeries, the total would still be very low. Very few patients with apnea have abnormal throats. However, all throats ARE DIFFERENT.
As someone who looks at throats for a living, I can tell you that throats are like faces. They are all similar, but they are all different. Some have large tongues, some small jaws, some low palates, some high palates, some narrow throats, some wide, but all are different.
Our throats are part of our physical anatomy given to us by our parents. It is our genetic gift for life. There are an infinite number of combinations that might be expected. The easiest way to describe the effects of our anatomy and genetics on our throats is simply by the throat’s size. Some throats are large and some are small. Smaller throats have less room for the relaxation that occurs during sleep and as a result, obstructive apnea may occur at a younger age. A large throat may result in one never having the condition.
Over the past fifty years there are a variety of diseases and conditions that have been recognized as producing Obstructive Sleep Apnea. Severe hypothyroidism and acromegaly are examples. These are rare causes. They affect muscle relaxation and airway size in a variety of ways. Some ethnic groups have been shown to have a higher incidence of Obstructive Sleep Apnea – predominately those of Southeast Asian and black heritage. These increases are proposed to be secondary to the bony structure of the face and cranium reducing airway size in those populations.
So these are the factors that lead to obstructive apnea: age, muscle relaxation, weight and genetics. By the time we are in our 70s, most of us will suffer from the condition. It could almost be considered a part of the aging condition. Add in the genetic component and the weight factor, obstructive apnea can appear at a younger age.
SUMMARY:
Three Predominate Components To
The Development Of Obstructive Sleep Apnea
Muscle relaxation – Increases with Age
Airway size – Genetics
Airway size – Weight
The combination of the above factors in some proportion leads to the development of obstructive sleep apnea for the majority of affected individuals.
It is best to think of Obstructive Sleep Apnea as a potential companion you will share for life. Like grey hair and glasses for most, hearing aids for some, obstructive sleep apnea is in your future. Once accepted and treated, it becomes just another of life’s companions and not a dreaded disease.