Yes, yes, Winston, I have heard about the new medication approved by the FDA. It has been heralded as the first drug approved for the treatment of Obstructive Sleep Apnea. “Is it so?” you ask. It is, but as an infamous man once said, “It all depends on what the definition of is, is.”
The approval is the FDA giving it an indication for use in obese patients with moderate to severe obstructive sleep apnea. With that approval, it becomes the first medication to have an indication for use in Obstructive Sleep Apnea. This is the fact that has been in multiple news outlets and led to many questions of sleep doctors by our patients. It is important to know more about the details.
The approval followed a multi-million dollar, manufacture sponsored study that was published in the New England Journal of Medicine (NEJM). The study focused on using the weight loss drug in obese individuals with Obstructive Sleep Apnea. Unsurprisingly, the weight loss induced by the medication resulted in improvement in the apnea condition. The treated patients were compared to those treated by diet alone who lost little weight during the study. It was not compared to other weight loss drugs. The article received wide acclaim and attention.
What was known about excessive body weight, weight loss and Obstructive Sleep Apnea before this study? I have an interest in the subject and have followed the work in the field since seeing my first patient with sleep apnea while serving in the Army. He was thin as a rail, by the way. Current knowledge is that we know slightly more than half of all newly diagnosed apnea patients have problems with their weight. We know that of those patients who experience significant weight loss, apnea is eliminated in 18-20% of the obese patients. The others are usually improved, but apnea is not eliminated.
My review of the NEJM article can be summarized briefly. The drug causes weight loss (previously known) and the weight loss improved apnea in many with it. Does it work any better than weight loss by any other means: diet, counseling or other weight loss drugs? Who knows? The study does not address the issue. Does it improve apnea over and above the effect of losing weight? Who knows? The study does not address the issue.
What did the article do? I don’t think it provided any new information. It most likely – I speculate here – influenced the FDA to add the Sleep Apnea with obesity indication to the medication’s approved usage. I suspect that the several million dollars spent for the study resulted in far more notoriety and media attention than any amount of advertising money could buy. Additional facts for you to consider are the cost of the medication and the duration of treatment it requires. A quick Internet search shows it to cost between 900 and 1,000 dollars a month on a well-known discount site. The duration of treatment is potentially life long.
No Winston, it is not proven to be a drug for apnea: just another very expensive drug for weight loss.
When we have medical problems, we all want to understand the ‘who’, ‘how’ and ‘why’ of the condition. Knowing may lead to changes or corrections that might fix and potentially remove the problem. Many professionals have invested their careers studying obstructive sleep apnea (OSA), trying to understand the ‘hows’ and ‘whys’ of OSA. It remains a subject that few professionals agree upon. Perhaps it’s best to review the broad landscape of OSA before we look at the details; reviewing the forest before the trees. Let’s look at the ‘who’ of OSA.
OSA is a common condition. How many people have it and what are their characteristics? We have a general outline for the answers to these questions and it is best to start with an understanding of those facts. First, how common is it?
Investigators have studied and reported answers to our questions, but the answers seem to change with each report. There are real reasons for the differing answers. Depending upon the how the information was obtained, the answers will vary. The source of the estimates can be from formal research designed to uncover the answer, population studies of many types, questionnaire reviews, insurance data reviews, or combinations of these and other techniques. The frequencies reported range from highs of 50% from Germany and 37% from Switzerland, to lows of 3% in Australia. When reviewing these reports, one is struck by the differences in how people were selected for inclusion in the studies; the variations in the definitions used to label someone as having OSA and by the increasing level of its reported occurrence as the years passed and the condition became more commonly known.
The differences in these reports are not hard to understand. Each has a specific method to gather potential individuals into the report. Enrollment into the study varies. In many reports, the individuals have to volunteer to provide private medical information. Even the report from closed medical populations in countries with government run medical systems cannot identify cases if the individuals do not participate. The wise blind man can only grasp what he can feel and the wise investigator can only see what he has chosen to look at.
Another factor to take into account is how the report defines ‘having OSA’. Are test results required? If so, what kind of test and what parameters are necessary to establish the diagnosis? What level of OSA does the study accept? Does it include what is generally considered to be mild OSA (5-15 apnea event per hour)? Does it require the higher level of moderate OSA (greater than 15 event per hour) or does it include both and how are they reported? Each report varies.
Many details chosen by investigators will determine the population they report and thus, the prevalence of the condition. Reviewing for this presentation, I went to the National Library of Medicine website to look for appropriate information. My search identified 10,388 articles with information about the prevalence of obstructive sleep apnea.
Prevalence is the frequency of occurrence of something (in this case obstructive sleep apnea) in a selected defined population.
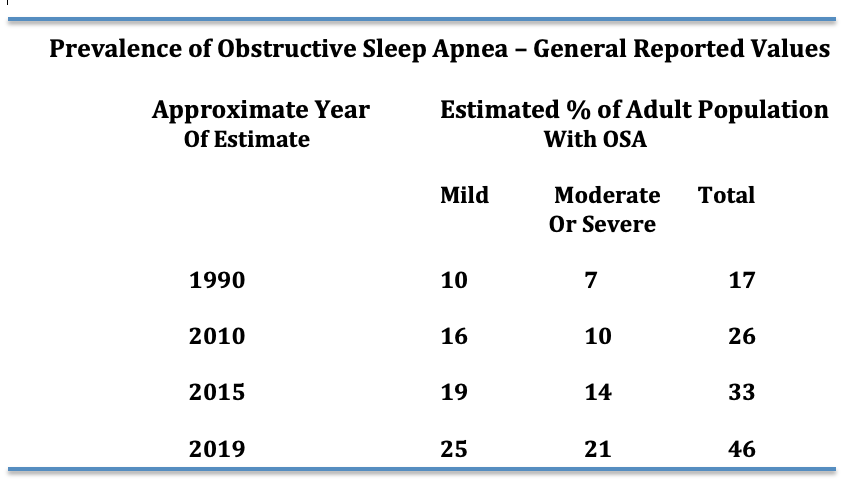
The important fact is that this condition is very common. How common is it? No consensus exists. The table below is constructed from several studies over the last 30 years and gives you an idea of reported values and how they have increased over the years.
I believe it is safe to say that at least 20 to 25% of adults in the United States have mild or greater apnea. Why the increase in prevalence with passing years? It is unclear, but most likely it represents the increase in awareness of the problem.
But, we need to be aware of still more details about who experiences OSA
Age is an important factor when measuring the prevalence of OSA. Few reports have elderly individuals participating. However, the report from Germany on 4,420 individuals from 20-81 years provides some answers. Half of the population had at least mild OSA and 20% had moderate or severe OSA. When broken down by age, 80% of men 70 y/o and older had some degree of OSA. The Swiss study also demonstrated a significant increase with age. Older studies do not show such a high prevalence in the elderly, but the majority of them did not include elderly individuals in the populations studied. Time will tell, but obstructive sleep apnea is very common in the elderly.
There is evidence that some ethnic groups may have more Obstructive Sleep Apnea than others. Particularly individuals of Southeast Asian or Black heritage. It is proposed that the cranial and facial boney structure in those groups leads to smaller upper airways.
What about occurrences during our youth and young adulthood? OSA is known to occur in infancy, childhood and during the teenage years. The prevalence for those ages is considered to be between 1 and 5%. As for early adulthood, there is substantial information from multiple reports to indicate it occurs in 5% to 8% of 18-30 year olds.
In the summary above I have used numbers that include both sexes. There is a significant difference in the occurrence of OSA between the sexes. In the report from Switzerland, 50% of men and 24% of women in the report had OSA. For most reports a significant difference between men and women is noted during the premenopausal years. With aging and menopause, the occurrence of OSA in women increases.
Summary – The Prevalence of Obstructive Sleep Apnea
The frequency increases with age in both sexes. After the age of 70, the occurrence rate is dramatic reaching up to 80% of adults in one study.
It is more common in men than women. After menopause the occurrence in females increases significantly
References:
Prevalence and association analysis of obstructive sleep apnea with gender and age differences. Fietze et al. J Sleep Res 2019 Oct; 28(5):e12770
Estimation of the global prevalence and burden of obstructive sleep apnea: a literature-based analysis. Benjafield et al. Lancet Respir Med. 2019Aug; 7(8):687-698
Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. R Henzer et al. Lancet Respir Med. 2015 Apr; 3(4): 310-318
Screening for Obstructive Sleep Apnea in Adults US Preventive Services Task Force Recommendation Statement. JAMA January 24/31 2017; 317(4) 407-414
Diagnosis and management of childhood obstructive sleep apnea syndrome. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, Schechter MS, Ward SD, Sheldon SH, Shiffman RN, Lehmann C, Spruyt K, American Academy of Pediatrics. Pediatrics. 2012;130(3):e714.
“Why am I using that this thing?” they asked me. This ‘thing’ they were referring to is also known as CPAP.
Many people find themselves having had a sleep test and they are not sure why. They have a CPAP machine (Constant Positive Airway Pressure machine). Yet, they tell me, “I don’t know why.” Yes, they’ve been told they have apnea (Obstructive Sleep Apnea or OSA), but why do they need to do this? It is a question that they should be able to answer. Why do we use CPAP? Why do we treat OSA?
Why do we treat OSA?
When a sleep evaluation or sleep testing was considered for you, your physician felt it might explain some of your sleep related symptoms or medical problems. It might have been for snoring that you were not even aware had been occurring. Maybe you were sleepier than you wanted to be or more sleepy than your family or friends thought you should be. It could have been for another non-related issue. Your doctor was concerned that your problem with glaucoma, asthma or hypertension may have been made worse by or possibly even caused by a sleep condition. The test was ordered. Obstructive Sleep Apnea was found and now you have a CPAP machine.
Obstructive Sleep Apnea may cause symptoms. Excessive sleepiness, poor quality nocturnal sleep and waking up with headaches are just a few of these symptoms. Your snoring could be waking your spouse. Certainly, you would prefer not to have the symptoms. You want to sleep better and to feel better during the day.
One of the major goals of therapy for OSA, including CPAP, is to improve or eliminate symptoms. When the obstructive apnea is corrected, many of its symptoms resolve or improve, sometimes dramatically. If you had symptoms when your apnea was diagnosed, one goal of therapy is to improve or correct those symptoms.
Most symptoms of OSA are not specific.
Most symptoms of OSA are not specific. A wide range of medical conditions, some common and others not so common, can cause these symptoms. It is unfortunate, but our sleepiness or headaches do not come with labels telling us what is causing them to occur. Often, sleep apnea treated with CPAP will totally correct the obstructive events, but the symptoms that led to the evaluation and testing do not go away.
Many patients at the time they are diagnosed with significant obstructive apnea will have few or no symptoms. These individuals have varying degrees of OSA severity on their sleep testing. Surprisingly, significant OSA can be seen with minimal symptoms or even no symptoms. While the number of obstructive events per hour will generally be related to the severity of the symptoms, is it not unusual to see patients with both moderate and severe apnea with few symptoms. Even without symptoms, our current knowledge strongly supports the need for their treatment.
Many patients at the time they are diagnosed with significant obstructive apnea will have few or no symptom.
Understanding the reason for treating individuals with few or no symptoms requires a little more information. Obstructive Sleep Apnea is the repeated interruption of someone’s breathing while asleep. The obstructions result in a blood oxygen drop and an arousal to light sleep or brief awaking. These arousals are not usually associated with full awakenings. Most individuals are not aware that the obstructions have occurred.
There are two types of obstructions. The first is a total blockage of the airway with a drop in blood oxygen level while breathing efforts from the chest continues. The technical term for complete obstruction is Apnea. The second is a partial blockage of the airway while the breathing continues. These partial blockages cause the same problems as seen with an apnea. The technical term for the partial obstruction is Hypopnea. The two types of obstruction are measured during a night or portion of a night of sleep testing. The numbers of each are added together. When divided by the duration of the sleep where the measurements were made, the results represent the number during an average hour of sleep. The resulting number is the Apnea-Hypopnea Index or AHI. The AHI is the average number of apneas and hypopneas in one hour of sleep.
The AHI is considered a measurement of the severity of Obstructive Sleep Apnea. Other factors enter into the measurement of severity. The most common would be the degree of oxygen drop that occurs with these obstructive events. It is generally accepted that an AHI of less than 5 is not considered to be diagnostic of OSA. An AHI of 5 to 15 events per hour is considered mild OSA. An AHI of 15 to 30 is moderate and above 30 is severe Obstructive Sleep Apnea.
The AHI is considered a measurement of the severity of Obstructive Sleep Apnea.
In the past 40 years, thousands of research studies on Obstructive Sleep Apnea have been performed. The vast majority utilize the severity scale noted above. Those studies strongly support the current concept of the role of apnea in causing and aggravating other medical conditions.
The higher a person’s AHI on their diagnostic sleep test, the more likely they will die from a stroke or heart attack. The risk is far higher than those who have no obstructive sleep apnea. And, they die younger. When the AHI is greater than 15 per hour the risk is significant. An increased risk is measurable at an AHI of five but it is relatively small. It is very small at an AHI of less than five. It is generally accepted the long-term treatment of patients with an AHI greater than 15 at the time of diagnosis will improve secondary medical conditions and prolong life.
The second goal of therapy is obvious. It is to reduce or eliminate as many apnea and hypopnea events as possible. A person with OSA cannot know what their AHI is on any given day, night, week or month. As noted above, the symptoms do not always reflect the success of OSA treatments. However, with modern CPAP machines, technology can measure those events (AHIs) while you use the machine. Reports are now available on most machines, on most machine manufacturer’s websites, or through your physician. You and your physician can know how well your therapy is controlling your AHI.
What have we covered.
1. Obstructive Sleep Apnea can occur with minimal or no symptoms.
2. Obstructive Sleep Apnea is treated for two reasons
3. Obstructive Sleep Apnea treatment may only improve one of the reasons it is being treated.
4. The Apnea Hypopnea Index (AHI) is the number of obstruction events per hour of sleep.The AHI while on therapy demonstrate how well the therapy is controlling the Obstructive Sleep Apnea.
Three questions follow naturally from this brief review. These topics will be addressed in future post.
1. Why do I still have symptoms on treatment for OSA?
2. If I have mild OSA when diagnosed, do I need treatment?
3. What is the definition of apnea?
Why is OSA treated? The two reasons are: to improve symptoms and control the obstructive events. When we treat OSA, the treatment may be successful treating both, or just one of the two. One or both may be the reason CPAP, or another treatment, was recommended for you.
Week four of our national shut down. Do you have your obstructive apnea under control? I hope this finds you healthy and sleeping well. What does having this virus around mean to you and others with obstructive sleep apnea?
Obstructive sleep apnea is a chronic condition. The coronavirus is a new infectious agent that produces a short-term illness. It is a respiratory infection and in many ways parallels influenza. It appears to be more contagious and may produces a more intense severe illness. None of us want to experience it.
Seasons and years come and go. Influenza comes and goes. The common cold is a frequent visitor to the lives of busy people. These things happen while people have the ongoing problem of obstructive sleep apnea. Now we can add coronavirus to the list.
Treatment Recommendations
Many aspects of our treatment recommendation are the same. The two most important are:
Continue to use your CPAP
Have a regular cleaning schedule for your equipment
A respiratory outbreak, certainly the current coronavirus episode, calls for some attention to treatment recommendations. While is it important to use the equipment, it is even more important to use your equipment during a widespread respiratory infections outbreak. Regular CPAP users have fewer respiratory illnesses during these community wide infectious episodes. While we do not have experience with the coronavirus, it seems likely that regular CPAP usage will help in a similar manner as it does with the usual respiratory illness. So by all means:
USE YOUR CPAP – All Night Every Night
Cleaning Recommendations
Special attention should be paid to cleaning your equipment. Sleep physicians are aware of the wide range of cleaning habits of our patients. Many of us do not follow the guidelines suggested by the manufactures. It might be time to reassess your cleaning pattern in the times of the coronavirus.
If you and yours are well and free of respiratory symptoms, cleaning your equipment should be on a fixed schedule. Mask, tubing and humidifier should be cleaned at least once a week. With a consideration of the nature of coronavirus, a dilute gentle soap solution would be the preferred cleaning agent. Soap is a superior agent for coronal virus disinfecting. If you haven’t been cleaning, start now.
KEEP YOUR EQUIPMENT CLEAN
What if you are diagnosed with, or suspected of having, the coronavirus?
Usage becomes even more important. When ill with respiratory symptoms, sleeping with your CPAP will speed up your recovery and lessen the severity of your illness. It is more important that ever that you use your CPAP during the illness.
Cleaning your equipment is more important. When you have the coronavirus infection it is best to clean your mask, tubing and humidifier daily. The machine and bedside table should be rubbed down with a disinfectant wipe. The pillowcase and sheets should be washed frequently if not daily. The room should be aired out daily, if possible, between sleeping hours.
What is sleep apnea? It is an extremely common condition that should be understood by everyone. Sleep apnea is a temporary blockage or obstruction of our breathing while we sleep. A person with sleep apnea experiences repeated blockages of their air passage during sleep. The condition of obstructive sleep apnea is diagnosed when the blockages occur repeatedly.
When we sleep, our muscles relax. This can result in significant narrowing and often closure of the air passage between the lungs and the mouth and nose. The obstruction occurs between the voice box (larynx) and the nasal passage and mouth. This relaxation results in a critical narrowing. At some degree of relaxation, as the passage narrows, air has difficulty passing in and out of our lungs. A partial obstruction is called ‘hypopnea’ while a complete obstruction is an ‘apnea’. Both hypopneas and apneas have the same effects. Each is a significant obstructive event.
Figure 1
Side view of anatomy of upper airway. Top figure shows normal open airway. The bottom figure shows area of obstruction during a obstructive apnea event. The obstruction demonstrated is at the base of the tongue
Obstruction of the airway leads to physiological changes. The level of oxygen in the blood drops and the level of carbon dioxide increases. These changes occur within a few seconds. The brain, through its mechanisms to control breathing, senses these changes and immediately increases our breathing efforts. The increased breathing effort results in the opening of the air passage and the return to normal of the blood oxygen and carbon dioxide levels. This increased effort often produces a loud noise, snore or snort as airway open. The blockage will last for 15 to 20 seconds on average. An individual can wake with the choking sensation when this occurs, however, that is very unusual. Most people sleep through the entire choking episode.
Figure 2
A three minute graphic recording of a person’s normal breathing. The items recorded are chest wall movements, air movement at nose and mouth, oxygen level, snoring and sleep level.
Figure 3
A three minute recording of a person having obstructive apnea events. Note the increase in chest wall movement, the absent of airflow, dropping oxygen levels, and snoring that is occurring.
The condition of obstructive sleep apnea is diagnosed when these events occur regularly and frequently. Current knowledge suggests that these have to occur at a certain frequency to create symptoms and/or medical problems. Medical professionals, insurance payers, and government bureaucrats established that five events or more per hour indicates the presence of the condition of obstructive sleep apnea.