Yes, I will try to answer your question. I understand your training has led you to believe that healthcare is a right. Why, you ask, did I pause before saying, “It’s not that simple. But if it were, the answer would have to be no.”
Consider first what is meant by the term, healthcare. Like most words, it is likely interpreted differently by almost everyone. The views will run from having clean water, a family doctor available for medical problems to those that would include anything to do with a person’s health. These are widely divergent categories of products and services based on different delivery systems and business models. It is almost impossible to discuss a ‘right to healthcare’ without understanding everything that is included in the discussion – the components of healthcare.
It is not the only term that needs to be defined. What do the promoters mean by the word, right? Maybe it is best to consider its meaning first.
When right is used as a noun, as it is in a ‘right to healthcare,’ common definitions according to Merriam-Webster include: qualities of moral correctness or moral propriety; something to which someone has a just claim; something to which someone may claim as their due; and, a cause of truth or justness. The proponents of a ‘right to healthcare’ usually mean the second or third of these definitions, a just claim or their due.
Healthcare has only one definition listed. Merriam-Webster defines it as ‘efforts to maintain or restore physical, mental or emotional well-being especially by trained or licensed professionals.’ Practically speaking, this definition would essentially cover all aspects of personal and public health. It would include the fields of preventive medicine, public health and personal medical care along with institutional medical care. Each of these fields is unique in how it is currently organized and delivered while sharing some common features. The shared features include the need for physical plants of operation, equipment to provide the services, support staff to carry out the services and a professional staff. These factors are needed in varying quantities and of different types for each of these fields of endeavors.
For clearer understanding we need to look more specifically at the services included in healthcare. These would include public health services, preventive medicine services (public or individual), individual’s urgent and chronic medical care, and institutional care (hospitalization and similar). We need to consider all the services that might be determined to be healthcare.
Public health is widely practiced throughout most local communities in our country. Public health services maintain and ensure clean water and adequate sewers, track communicable diseases and advise the population about those diseases. Their services, physical plant, equipment, staff and professionals are paid for and employed by government units. They are paid for by taxes and by fees for water and sewer services. For the majority of urban areas in this country, these health services are for all practical purposes already a right provided by the government. Certainly, there are exceptions for rural and smaller communities, but most citizens already enjoy public health as a government service. Paid for by their taxes.
Preventive medical services are currently provided by both government operations and individual medical providers. Examples of government services include monitoring of new and current medications for problems, providing recommendations for vaccinations, and monitoring of medical devices. Again, the facilities, staff, equipment and professionals are supplied and paid for by the government taxes and fees usually paid by the businesses for the service.
At a more personal level, physicians, providers, healthcare businesses and employers (insurance companies, medical practices, clinics, hospitals and businesses) may provide guidance and assistance on preventive medical measures that an individual needs. These businesses provide the physical plant, staff, equipment and professional organization needed. The expense for these services is recouped through fees, insurance payment, employers and other methods. The healthcare provided at this level is the first at which an individual may be responsible for all or part of the cost of the services.
The next component leads further into individual responsibility, providing an individual’s urgent and ongoing medical care. This is the form of healthcare we are familiar with and what is most often thought of when discussing ‘a right to healthcare’. In our country’s history, these services have been provided by individual professionals who own and operate their own businesses. Recent change in economics, economic policy and legal structures of medical businesses has led to more large organizations (hospitals and insurance companies) owning more of these types of businesses. In these operations in any form, the expenses – from cotton swabs to physician income – are paid for by individuals, either directly or through surrogates (employers, insurances or others).
An individual’s surrogates are the primary payees for the institutional care portion of our healthcare delivery system. This portion of healthcare, hospitalization primarily, is where the largest cost (facilities, equipment, staff and professionals) occurs. Again, most of the cost is paid for by individuals or their surrogates.
In these areas of healthcare where the individual is mostly responsible for the cost of the service, there is one major group of individuals that is not responsible directly. Those are individuals on government insurance such as Medicare. In Medicare and other government plans, a person may have a markedly reduced or no exposure to the direct cost of the services. Those who argue for a ‘right to healthcare” would like all services for all citizens to be paid for by the government.
My comments have gone on long enough so I will save my additional thoughts for a future letter. I would add in closing what I think summarizes the whole question.
A ‘right to healthcare’ should mean everyone has access to and freedom to decide how to obtain their healthcare. At present, I would argue that it is already the case, but it is disappearing rapidly. In reality, the discussion is not about freedom to get healthcare, but getting healthcare for free.
Yes, I received your note. I apologize for my delay in setting this up. Your idea to post these so you can keep track of them was a good one. I will select a few of my past notes and post them here for you.
I found the first of my letters. We will start with it.
RGH August 1, 2022
Winston
It will seem strange to receive this from me, as we have not talk seriously except on rare occasions. I have been a family friend beginning decades before your birth. Now, you are away from home with a new wife, pursuing a medical education. A calling I have followed for more decades than I have known your family. It is a difficult master with challenging hurtles and responsibilities that each of us experience differently.
Our interactions are few and infrequent, intermingled with talk from family and friends on special occasions and holidays. Meaningful thoughts don’t seem to reach across the table or room. Medical or should I say professional conversations often by there nature are inappropriate in those situations. So, I have returned to the written word to communicate my beliefs, attitudes and some would say prejudices developed over my 50 years in medicine as first a doctor and now as a physician.
Do not be surprised by the letters or the subjects. You may respond with your questions and thoughts, but do not feel obliged. They represent an attempt to pass to you some little perspective on your chosen profession.
Ref: Rat Journals, Sturgeon’s Law and the Hawkins’ Corollary
Yes, I know I have mentioned Hawkins’ Law to you many times. And yes, you need to know what I mean. I will answer that for you with a little background. Have you heard of Sturgeon’s Law?
Sturgeon’s Law “Ninety percent of everything is crap”
Corollary 1: “The existence of immense quantities of trash in science fiction is admitted and it is regrettable: but it is no more unnatural than the existence of trash anywhere.”
Corollary 2: “The best science fiction is as good as the best fiction in any field.”
Sturgeon was, early in his career, a science fiction writer and an editor of a science fiction magazine. He received intense criticism for the quality of writing in science fiction and his response was what was to become known as Sturgeon’s Law. References point out that others have had similar insights.
Voltaire in a short story, “… but in all times, in all countries, and in all genres, the bad abounds, and the good is rare.”
Rudyard Kipling in the ‘The Light that Failed’, “Four-fifths of everybody’s work must be bad. But the remnant is worth the trouble for its own sake.”
George Orwell in ‘Confessions of a book reviewer’, ‘In much more than nine cases out of ten, the only objectively truthful criticism would be “ This book is worthless”.’
I initially encountered Joseph Hawkins, M.D, when I was first year resident in internal medicine at the University of Oklahoma. At that time, Joe was the Consultant to the Army Surgeon General who oversaw assignments of duty stations for doctors going on active duty. I was a recent draftee about to enter the US Army.
Someone I knew in the Army had given me his name and the number of his office in Washington. I called him about my potential assignment on entering the Army, hoping not to go to Vietnam. When I advised him that I would be a partially trained internal medicine specialist when I went on active duty and suggested I might be valuable at a major hospital, he laughed. Joe gave me some sage advice. He said I should consider entering an Army medical residency program to complete my training. Probably the best advice I have ever been offered in my entire medical career.
Over a decade later, Joe and I found ourselves in Phoenix, in adjacent hospitals, in the same specialty – Pulmonary and Critical Care Medicine. He was the director of fellowship training for our specialty at a regional teaching hospital and I was the director of the Pulmonary, Sleep and Critical Care services, at a hospital that helped with their training programs. We shared training fellows and clinical experiences till his retirement.
At our monthly journal club meetings, Joe would frequently ask. “What does the Rat journal have in it this month?” One of our leading specialty journals had become focused on basic science research, departing from its decades long tradition of clinical based reporting. For a time it frequently involved rats. The journal became known to our group as the Rat Journal. Practically all of its publications had little to do with the practice of medicine and most had little to do with significant advancements in sciences.
I believe the growing volume of medical literature is, and possible always has been, of little practical or insight value. I would call it Hawkins’ Law or the Hawkins’ corollary to Sturgeon’s Law: Ninety percent of medical research is crap.
As physicians, it is our burden and task to sort the information overload and find the 10%. A firm foundation is needed in what is generally accepted knowledge, (knowing the current basic understanding of the medical disease, issue or problem) to judge how a new piece of information alters, changes or discounts our basic understanding. Remember that the understanding of all human diseases will be further defined, changed, or altered during your medical career.
There are complex airway dynamics resulting in blockage of the upper airway producing Obstructive Sleep Apnea. Although complex, the process can be viewed in a general non-technical manner to help one understand the causes of obstructive sleep apnea.
In such an overview, we find two components to the events producing blockage of the airway during sleep: airway muscle relaxation and airway size. How does each of these contribute to the development of obstructive apnea?
The basic event of sleep apnea is the relaxation of the upper airway (the throat above the Adam’s apple to the nose and mouth) narrowing it critically or totally, resulting in a blockage limiting the amount of air traveling into or out of the lungs. This causes a drop in the blood oxygen and an increase in the blood carbon dioxide. These are changes, which the brain notices immediately. The very next breathing effort by the diaphragm is stronger. These efforts keep increasing until two or three breaths later, on average about 15 to 20 seconds, the effort is strong enough that the throat opens and air moves in and out again. Commonly, but certainly not always, this is accompanied by a loud snore or snort. These events are what produce Obstructive Sleep Apnea.
While these events alone may not be medically important, they produce problems when they occur repeatedly. A measurement of five events per hour while sleeping is considered diagnostic of Obstructive Sleep Apnea in the United States. Problems are thought to develop at this point.
Relaxation of the tongue and pharyngeal muscles play a role in developing these events. As we age, muscle tone decreases. Strength reduces. Tissue tone becomes slack, to say the least. We have all seen the effects of age in our family, friends and maybe even ourselves. The same changes take place in our tongue, pharyngeal muscles and supporting tissues. The prevalence data for obstructive sleep apnea show a steady increase with age. Those greater than 70 years of age are reported to have an 80% frequency of occurrence.
Muscle relaxation and muscle changes with age are major components of the causation of obstructive apnea.
What role does airway size play in causing obstructive apnea? The size of the airway determines how much muscle relaxation is needed for the critical narrowing to occur. Smaller airways will close more easily than larger ones
It is best to look at the airway size as two issues – weight and genetics.
In the 1960s, doctors discovered and described the obstructive apnea problem in obese patients. For the first 20 years after its description, many strongly believed that obstructive apnea was just a complication of obesity, not an independent problem. When a person gains weight, the fat tissue is added over the muscles below the skin in most areas of the body, including under the skin in the throat. The accumulation in the throat makes the size of the airway smaller. With a smaller airway, less relaxation is required to cause the critical narrowing resulting in an obstructive apnea event.
It is now well known that at certain weights almost everyone will have apnea. The medical community uses a measurement that is a calculation based on height and weight. This is called the Body Mass Index or BMI. A normal BMI is 20 to 25. When a person’s BMI reaches 40, ninety percent of those individuals will have sleep apnea.
Obesity can cause sleep apnea. What is its contribution to all those individuals with the condition? No one agrees and there has been ongoing debate since the 1970s.
Like most medical controversies, variation in the reported studies makes the issue more difficult to understand.
Early attempts to understand the effects of weight loss on apnea used an improvement in symptoms as the mark of correcting the problem. When obese patients with apnea lose a significant amount of weight, they feel and sleep better. The authors of those reports concluded that obstructive sleep apnea was cured by weight loss. But, did it really cure the apnea?
As more studies were done, the investigators began testing for apnea after weight loss. To assess the effect of weight loss on correcting apnea, the reports used changes in patients’ sleep test measurements. Typically, they would use a percentage drop in the number of apnea events or select a set level of events at 15 or 5 per hour. The level of 5 is the diagnostic level accepted for the diagnosis of the condition. These studies report a high level of symptomatic improvement with weight loss. Unfortunately, only 10-15% of obese patients will drop their levels below 5 after weight loss. Most will reduce the number of events limiting the severity, but few can be considered as cured. For an individual, weight loss can have significant beneficial effects on treatment, need for treatment and symptoms. However, when viewed as a cause, few can be considered to have obstructive apnea caused by obesity.
My experience reported a few years ago at a community sleep center gives an insight. For every one hundred cases of newly diagnosed obstructive sleep apnea, 60 will have BMIs in the obese range, meaning that 60% were obese. After weight loss, we know only 10 to 15% of individuals will have their apnea event drop below 5 per hour. In the one hundred newly diagnosed individuals with apnea, weight loss will correct the apnea in only 6-10 of the 60 who had weight issues. The other 50- 54 previously obese now are of normal weight and still have apnea. They will feel better after weight loss, but they will still have apnea. There are now a total of approximately 90 who still have apnea. Why?
There is the problem of muscle relaxation of course, but there is the other component of airway size – Genetics.
Sleep doctors look at throats when evaluating their patients. As a practitioner for many years, I have looked at the throats of thousands of patients with obstructive apnea. How many abnormal throats have I observed? Not many. I have seen one throat malignancy in my last two thousand exams. By including enlarged tonsils and changes due to prior surgeries, the total would still be very low. Very few patients with apnea have abnormal throats. However, all throats ARE DIFFERENT.
As someone who looks at throats for a living, I can tell you that throats are like faces. They are all similar, but they are all different. Some have large tongues, some small jaws, some low palates, some high palates, some narrow throats, some wide, but all are different.
Our throats are part of our physical anatomy given to us by our parents. It is our genetic gift for life. There are an infinite number of combinations that might be expected. The easiest way to describe the effects of our anatomy and genetics on our throats is simply by the throat’s size. Some throats are large and some are small. Smaller throats have less room for the relaxation that occurs during sleep and as a result, obstructive apnea may occur at a younger age. A large throat may result in one never having the condition.
Over the past fifty years there are a variety of diseases and conditions that have been recognized as producing Obstructive Sleep Apnea. Severe hypothyroidism and acromegaly are examples. These are rare causes. They affect muscle relaxation and airway size in a variety of ways. Some ethnic groups have been shown to have a higher incidence of Obstructive Sleep Apnea – predominately those of Southeast Asian and black heritage. These increases are proposed to be secondary to the bony structure of the face and cranium reducing airway size in those populations.
So these are the factors that lead to obstructive apnea: age, muscle relaxation, weight and genetics. By the time we are in our 70s, most of us will suffer from the condition. It could almost be considered a part of the aging condition. Add in the genetic component and the weight factor, obstructive apnea can appear at a younger age.
SUMMARY:
Three Predominate Components To
The Development Of Obstructive Sleep Apnea
Muscle relaxation – Increases with Age
Airway size – Genetics
Airway size – Weight
The combination of the above factors in some proportion leads to the development of obstructive sleep apnea for the majority of affected individuals.
It is best to think of Obstructive Sleep Apnea as a potential companion you will share for life. Like grey hair and glasses for most, hearing aids for some, obstructive sleep apnea is in your future. Once accepted and treated, it becomes just another of life’s companions and not a dreaded disease.
When we have medical problems, we all want to understand the ‘who’, ‘how’ and ‘why’ of the condition. Knowing may lead to changes or corrections that might fix and potentially remove the problem. Many professionals have invested their careers studying obstructive sleep apnea (OSA), trying to understand the ‘hows’ and ‘whys’ of OSA. It remains a subject that few professionals agree upon. Perhaps it’s best to review the broad landscape of OSA before we look at the details; reviewing the forest before the trees. Let’s look at the ‘who’ of OSA.
OSA is a common condition. How many people have it and what are their characteristics? We have a general outline for the answers to these questions and it is best to start with an understanding of those facts. First, how common is it?
Investigators have studied and reported answers to our questions, but the answers seem to change with each report. There are real reasons for the differing answers. Depending upon the how the information was obtained, the answers will vary. The source of the estimates can be from formal research designed to uncover the answer, population studies of many types, questionnaire reviews, insurance data reviews, or combinations of these and other techniques. The frequencies reported range from highs of 50% from Germany and 37% from Switzerland, to lows of 3% in Australia. When reviewing these reports, one is struck by the differences in how people were selected for inclusion in the studies; the variations in the definitions used to label someone as having OSA and by the increasing level of its reported occurrence as the years passed and the condition became more commonly known.
The differences in these reports are not hard to understand. Each has a specific method to gather potential individuals into the report. Enrollment into the study varies. In many reports, the individuals have to volunteer to provide private medical information. Even the report from closed medical populations in countries with government run medical systems cannot identify cases if the individuals do not participate. The wise blind man can only grasp what he can feel and the wise investigator can only see what he has chosen to look at.
Another factor to take into account is how the report defines ‘having OSA’. Are test results required? If so, what kind of test and what parameters are necessary to establish the diagnosis? What level of OSA does the study accept? Does it include what is generally considered to be mild OSA (5-15 apnea event per hour)? Does it require the higher level of moderate OSA (greater than 15 event per hour) or does it include both and how are they reported? Each report varies.
Many details chosen by investigators will determine the population they report and thus, the prevalence of the condition. Reviewing for this presentation, I went to the National Library of Medicine website to look for appropriate information. My search identified 10,388 articles with information about the prevalence of obstructive sleep apnea.
Prevalence is the frequency of occurrence of something (in this case obstructive sleep apnea) in a selected defined population.
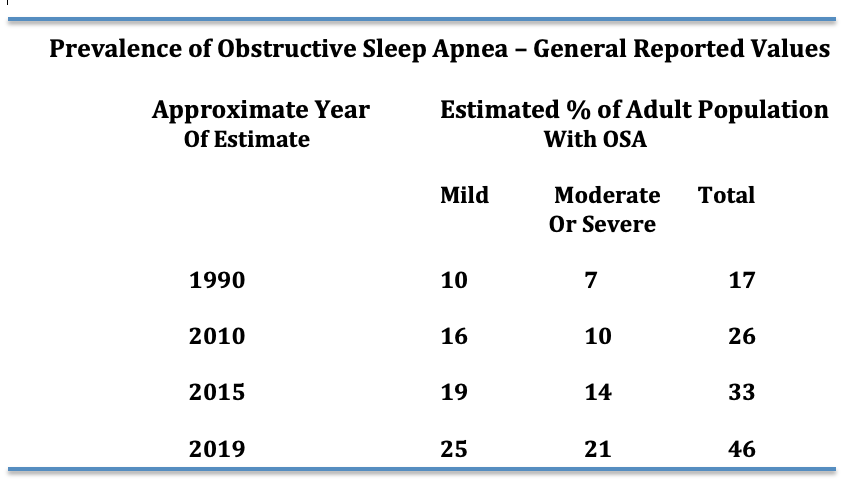
The important fact is that this condition is very common. How common is it? No consensus exists. The table below is constructed from several studies over the last 30 years and gives you an idea of reported values and how they have increased over the years.
I believe it is safe to say that at least 20 to 25% of adults in the United States have mild or greater apnea. Why the increase in prevalence with passing years? It is unclear, but most likely it represents the increase in awareness of the problem.
But, we need to be aware of still more details about who experiences OSA
Age is an important factor when measuring the prevalence of OSA. Few reports have elderly individuals participating. However, the report from Germany on 4,420 individuals from 20-81 years provides some answers. Half of the population had at least mild OSA and 20% had moderate or severe OSA. When broken down by age, 80% of men 70 y/o and older had some degree of OSA. The Swiss study also demonstrated a significant increase with age. Older studies do not show such a high prevalence in the elderly, but the majority of them did not include elderly individuals in the populations studied. Time will tell, but obstructive sleep apnea is very common in the elderly.
There is evidence that some ethnic groups may have more Obstructive Sleep Apnea than others. Particularly individuals of Southeast Asian or Black heritage. It is proposed that the cranial and facial boney structure in those groups leads to smaller upper airways.
What about occurrences during our youth and young adulthood? OSA is known to occur in infancy, childhood and during the teenage years. The prevalence for those ages is considered to be between 1 and 5%. As for early adulthood, there is substantial information from multiple reports to indicate it occurs in 5% to 8% of 18-30 year olds.
In the summary above I have used numbers that include both sexes. There is a significant difference in the occurrence of OSA between the sexes. In the report from Switzerland, 50% of men and 24% of women in the report had OSA. For most reports a significant difference between men and women is noted during the premenopausal years. With aging and menopause, the occurrence of OSA in women increases.
Summary – The Prevalence of Obstructive Sleep Apnea
The frequency increases with age in both sexes. After the age of 70, the occurrence rate is dramatic reaching up to 80% of adults in one study.
It is more common in men than women. After menopause the occurrence in females increases significantly
References:
Prevalence and association analysis of obstructive sleep apnea with gender and age differences. Fietze et al. J Sleep Res 2019 Oct; 28(5):e12770
Estimation of the global prevalence and burden of obstructive sleep apnea: a literature-based analysis. Benjafield et al. Lancet Respir Med. 2019Aug; 7(8):687-698
Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. R Henzer et al. Lancet Respir Med. 2015 Apr; 3(4): 310-318
Screening for Obstructive Sleep Apnea in Adults US Preventive Services Task Force Recommendation Statement. JAMA January 24/31 2017; 317(4) 407-414
Diagnosis and management of childhood obstructive sleep apnea syndrome. Marcus CL, Brooks LJ, Draper KA, Gozal D, Halbower AC, Jones J, Schechter MS, Ward SD, Sheldon SH, Shiffman RN, Lehmann C, Spruyt K, American Academy of Pediatrics. Pediatrics. 2012;130(3):e714.